
Once you open the online editor for PDFs by FormsPal, it is easy to complete or edit ca workshare program right here. To retain our editor on the cutting edge of convenience, we strive to integrate user-driven capabilities and improvements regularly. We are routinely grateful for any suggestions - help us with remolding how you work with PDF files. With just a couple of basic steps, you'll be able to start your PDF journey:
Step 1: Open the PDF file in our editor by clicking the "Get Form Button" at the top of this page.
Step 2: The editor will let you change PDF forms in various ways. Transform it by writing your own text, correct existing content, and put in a signature - all within the reach of a few clicks!
This form will require specific details to be entered, thus be sure to take your time to type in what's asked:
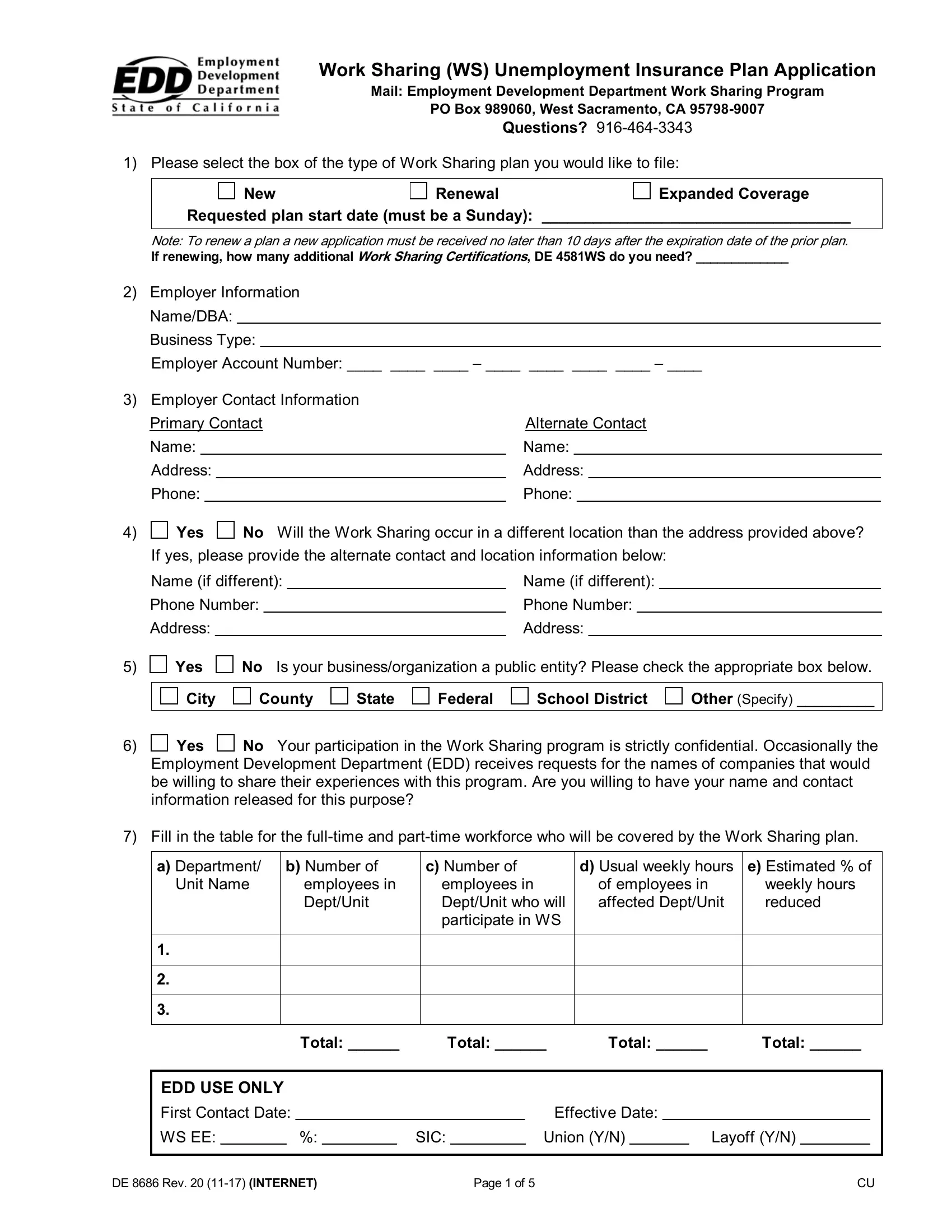
1. You need to fill out the ca workshare program accurately, therefore take care when filling out the parts including all these blanks:
2. When the last part is completed, you should include the necessary specifics in Yes, No Is your businessorganization a, City, County, State, Federal, School District, Other Specify, Yes, No Your participation in the Work, Employment Development Department, Fill in the table for the, a Department, b Number of, and c Number of in order to move forward to the next part.
3. The next step is going to be straightforward - fill out all the form fields in Check the box below with the, Weekly, Biweekly, Monthly, Other Specify, If your pay period is weekly or, Mon, Tues, Wed, Thur, Fri, Sat, Sun, Yes, and No If you were not approved to to complete the current step.
4. The next part requires your details in the subsequent parts: If yes the below sections must be, Union Name, Union Local Number, Phone Number, Name of Authorized Union, Authorized Union Representative, Position Title, Date, Union Name, Union Local Number, Phone Number, Name of Authorized Union, Authorized Union Representative, Position Title, and Date. Be sure you provide all of the requested info to go onward.
Be extremely attentive while filling in Phone Number and If yes the below sections must be, as this is the part where most people make some mistakes.
5. The pdf should be wrapped up with this section. Below you will notice a full listing of blank fields that require specific information for your document submission to be complete: who are not participating in the, Yes, No Will a reduction in, the WS plan If yes answer the, Yes, No If so will those reductions be, who are not participating in the, DE Rev INTERNET, and Page of.

Step 3: Revise the details you've inserted in the blank fields and then click on the "Done" button. Acquire the ca workshare program the instant you join for a free trial. Immediately access the pdf form from your personal account page, with any edits and adjustments being conveniently preserved! FormsPal offers safe form tools with no personal data recording or distributing. Feel comfortable knowing that your information is in good hands here!