
The purpose supporting our PDF editor was to make certain it is as straightforward as possible. You'll find the complete process of completing edd 2501 pdf rather simple when you adhere to all of these steps.
Step 1: Select the button "Get Form Here" on the site and press it.
Step 2: Now, you're on the document editing page. You may add content, edit present details, highlight specific words or phrases, put crosses or checks, add images, sign the document, erase unnecessary fields, etc.
The PDF form you are going to create will consist of the next parts:
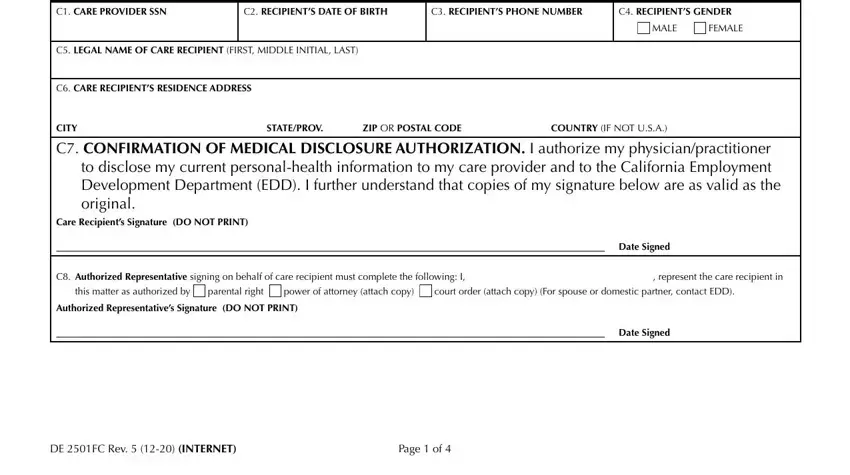
Enter the required details in PART, C, STATEMENT, OF, CARE, RECIPIENT CC, ARE, PROVIDERS, SN C, RECIPIENTS, DATEOFBIRTH C, RECIPIENTS, PHONE, NUMBER C, RECIPIENTS, GENDER MALE, FEMALE, CC, ARE, RECIPIENTS, RESIDENCE, ADDRESS STATE, PRO, V ZIP, OR, POSTAL, CODE COUNTRY, IF, NOT, USA Care, Recipients, Signature, DO, NOT, PRINT Date, Signed represent, the, care, recipient, in and this, matter, as, authorized, by section.
You should identify the significant details from the LEFT, BLANK, INTENTIONALLY and Enter, your, receipt, number, here field.
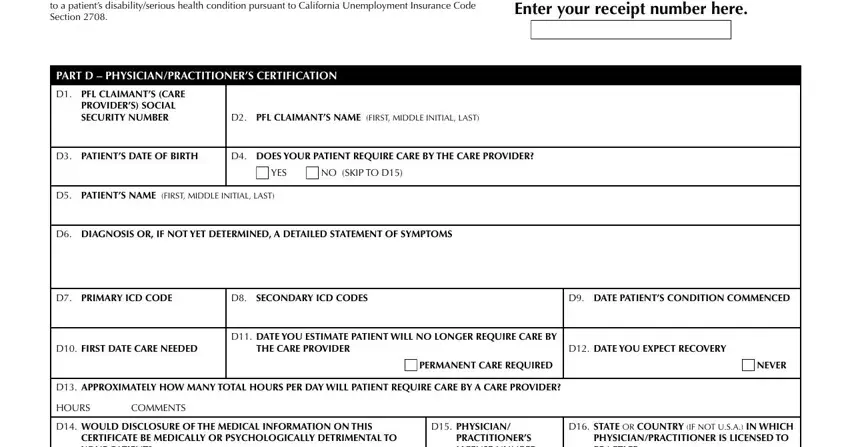
The Enter, your, receipt, number, here PROVIDERS, SOCIAL, SECURITY, NUMBER D, PATIENTS, DATEOFBIRTH YES, NO, SKIP, TOD D, PATIENTS, NAME, FIRST, MIDDLE, INITIAL, LAST D, PRIMARY, ICD, CODE D, SECONDARY, ICD, CODES D, DATE, PATIENTS, CONDITION, COMMENCED D, FIRST, DATE, CARE, NEEDED THE, CARE, PROVIDER D, DATE, YOU, EXPECT, RECOVERY PERMANENT, CARE, REQUIRED NEVER, and HOURS box can be used to specify the rights and obligations of both sides.
Review the fields PRACTITIONERS, LICENSE, NUMBER YES, CITY, STATE, PRO, V ZIP, OR, POSTAL, CODE COUNTRY, IF, NOT, USA D, TYPE, OF, PHYSICIAN, PRACTITIONER D, SPECIALTY, IF, ANY PHYSICIAN, PRACTITIONERS, PHONE, NUMBER and DATE, SIGNED and next fill them in.
Step 3: Hit the "Done" button. Next, it is possible to transfer your PDF document - upload it to your device or forward it by using email.
Step 4: Make sure you stay clear of possible future misunderstandings by generating as much as 2 copies of your document.
