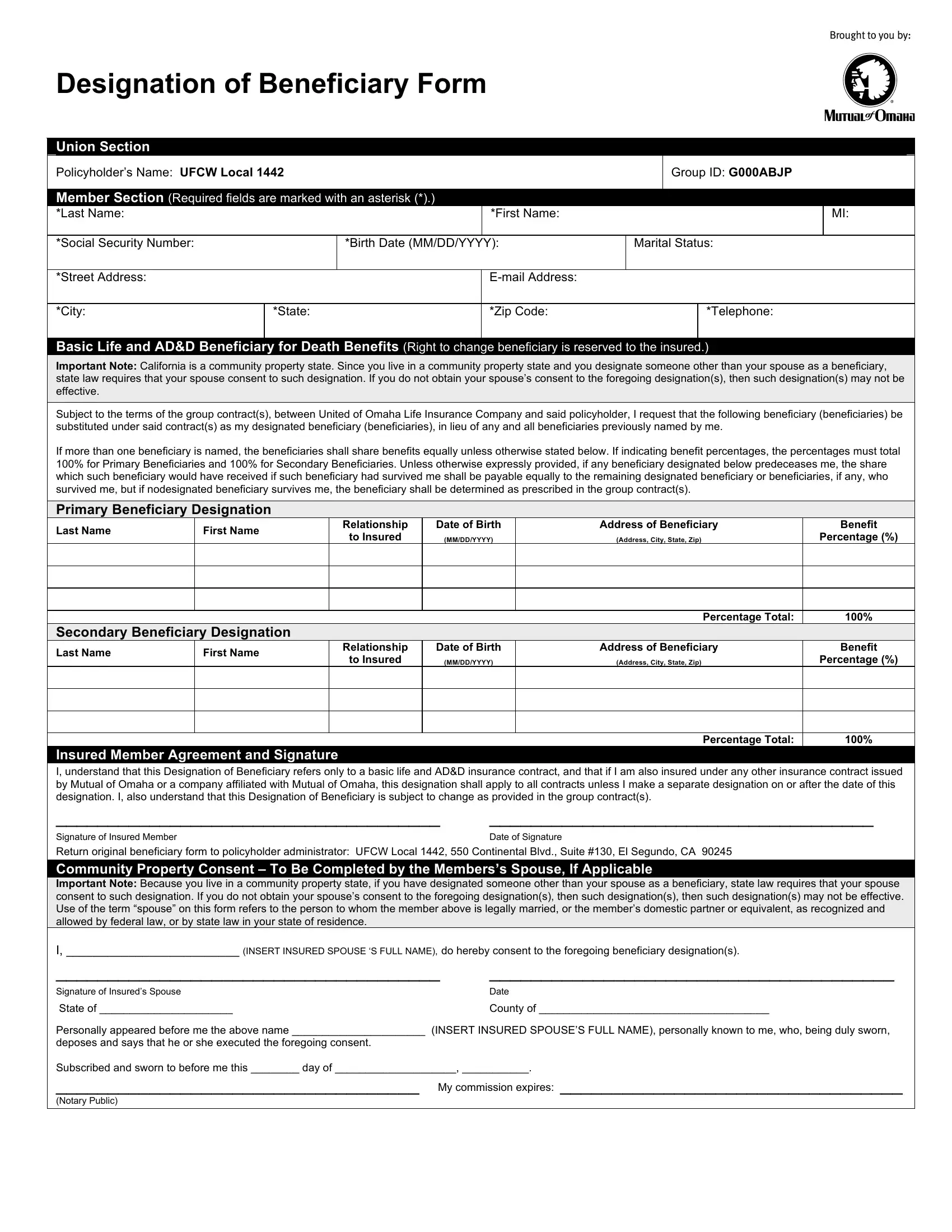
When it comes to preparing for the future, completing a Designation of Beneficiary Form is one of the most crucial steps anyone with a life and accidental death and dismemberment (AD&D) insurance policy can take. This form, essential for UFCW Local 1442 policyholders, ensures that the benefits from these policies are directed according to the policyholder's wishes in the event of their death. It mandates the policyholder to provide detailed information including names, relationships to the insured, and the allocation of benefits among primary and secondary beneficiaries—instructing that the shares be divided equally unless stated otherwise. Additionally, in places like California, being a community property state, it becomes necessary to obtain the spouse's consent if the beneficiary designated is someone other than the spouse. This condition underscores the importance of understanding local laws' impact on such designations. Addressing each required field, marked with an asterisk for emphasis, the form becomes a testament to how policyholders envisage the support of their loved ones after they are gone. Furthermore, the option for policyholders to specify different beneficiaries for other insurance contracts highlights the form's adaptability to the insured's comprehensive estate planning needs. With the inclusion of an agreement and signature section, along with a space for community property state consent from the spouse, the form encapsulates a full spectrum of considerations, making it a pivotal document for policyholders and their families.
| Question | Answer |
|---|---|
| Form Name | Designation Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | printable blank car title, what to fill in designation for students, mutual omaha beneficiary form, make a temporary tag |
Designation of Beneficiary Form
Union Section
Policyholder’s Name: UFCW Local 1442 |
|
|
|
Group ID: G000ABJP |
|||
|
|
|
|
|
|
|
|
Member Section (Required fields are marked with an asterisk (*).) |
|
|
|
|
|||
*Last Name: |
|
|
*First Name: |
|
|
|
MI: |
|
|
|
|
|
|
|
|
*Social Security Number: |
|
*Birth Date (MM/DD/YYYY): |
Marital Status: |
||||
|
|
|
|
|
|
|
|
*Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*City: |
*State: |
|
*Zip Code: |
|
|
*Telephone: |
|
|
|
|
|
|
|
|
|
Basic Life and AD&D Beneficiary for Death Benefits (Right to change beneficiary is reserved to the insured.)
Important Note: California is a community property state. Since you live in a community property state and you designate someone other than your spouse as a beneficiary, state law requires that your spouse consent to such designation. If you do not obtain your spouse’s consent to the foregoing designation(s), then such designation(s) may not be effective.
Subject to the terms of the group contract(s), between United of Omaha Life Insurance Company and said policyholder, I request that the following beneficiary (beneficiaries) be substituted under said contract(s) as my designated beneficiary (beneficiaries), in lieu of any and all beneficiaries previously named by me.
If more than one beneficiary is named, the beneficiaries shall share benefits equally unless otherwise stated below. If indicating benefit percentages, the percentages must total 100% for Primary Beneficiaries and 100% for Secondary Beneficiaries. Unless otherwise expressly provided, if any beneficiary designated below predeceases me, the share which such beneficiary would have received if such beneficiary had survived me shall be payable equally to the remaining designated beneficiary or beneficiaries, if any, who survived me, but if nodesignated beneficiary survives me, the beneficiary shall be determined as prescribed in the group contract(s).
Primary Beneficiary Designation
Last Name
First Name
Relationship |
Date of Birth |
to Insured |
(MM/DD/YYYY) |
|
|
Address of Beneficiary
(Address, City, State, Zip)
Benefit
Percentage (%)
Percentage Total:
100%
Secondary Beneficiary Designation
Last Name
First Name
Relationship |
Date of Birth |
to Insured |
(MM/DD/YYYY) |
|
|
Address of Beneficiary
(Address, City, State, Zip)
Benefit
Percentage (%)
Percentage Total:
100%
Insured Member Agreement and Signature
I, understand that this Designation of Beneficiary refers only to a basic life and AD&D insurance contract, and that if I am also insured under any other insurance contract issued by Mutual of Omaha or a company affiliated with Mutual of Omaha, this designation shall apply to all contracts unless I make a separate designation on or after the date of this designation. I, also understand that this Designation of Beneficiary is subject to change as provided in the group contract(s).
_____________________________________ |
_____________________________________ |
Signature of Insured Member |
Date of Signature |
Return original beneficiary form to policyholder administrator: UFCW Local 1442, 550 Continental Blvd., Suite #130, El Segundo, CA 90245
Community Property Consent – To Be Completed by the Members’s Spouse, If Applicable
Important Note: Because you live in a community property state, if you have designated someone other than your spouse as a beneficiary, state law requires that your spouse consent to such designation. If you do not obtain your spouse’s consent to the foregoing designation(s), then such designation(s), then such designation(s) may not be effective. Use of the term “spouse” on this form refers to the person to whom the member above is legally married, or the member’s domestic partner or equivalent, as recognized and allowed by federal law, or by state law in your state of residence.
I, _________________________ (INSERT INSURED SPOUSE ‘S FULL NAME), do hereby consent to the foregoing beneficiary designation(s).
_____________________________________ |
_______________________________________ |
Signature of Insured’s Spouse |
Date |
State of ______________________ |
County of ______________________________________ |
Personally appeared before me the above name ______________________ (INSERT INSURED SPOUSE’S FULL NAME), personally known to me, who, being duly sworn,
deposes and says that he or she executed the foregoing consent.
Subscribed and sworn to before me this ________ day of ____________________, ___________.
___________________________________ My commission expires: _________________________________
(Notary Public)