
You may work with 5-month without difficulty using our online PDF tool. FormsPal is aimed at providing you the perfect experience with our editor by consistently adding new functions and improvements. Our editor has become even more helpful with the most recent updates! At this point, working with PDF documents is simpler and faster than ever. If you are seeking to get started, here's what it will require:
Step 1: Click on the "Get Form" button at the top of this webpage to get into our PDF editor.
Step 2: With the help of our advanced PDF file editor, it's possible to accomplish more than simply complete blank fields. Edit away and make your documents seem perfect with custom text added in, or adjust the original input to excellence - all that comes with an ability to insert your personal graphics and sign the document off.
Be mindful when filling out this form. Make certain each field is completed correctly.
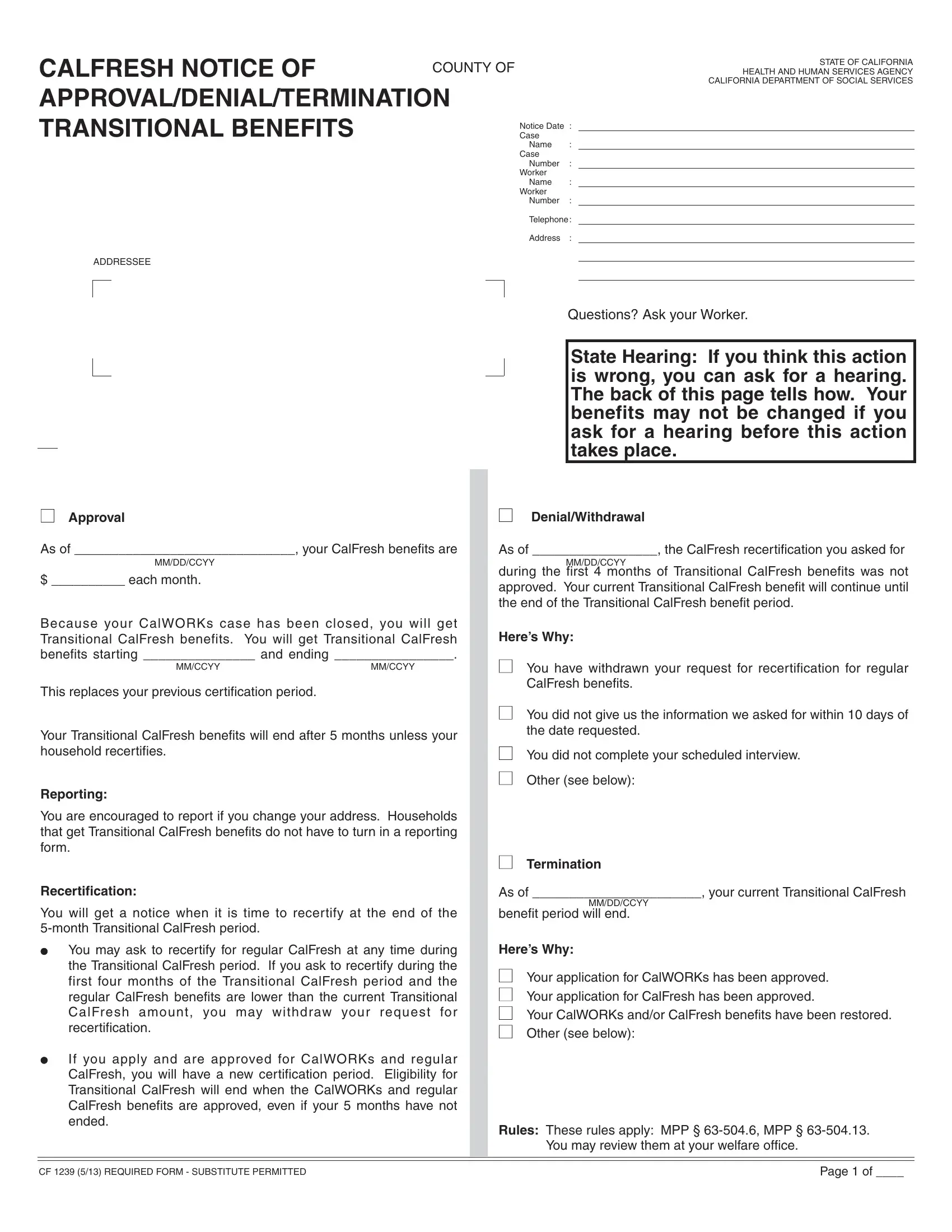
1. You'll want to fill out the 5-month accurately, so be careful when working with the sections containing these specific blank fields:
2. Immediately after the first array of fields is completed, go on to type in the relevant information in these - Approval, DenialWithdrawal, As of your CalFresh benefits are, As of the CalFresh, each month, MMDDCCYY, Because your CalWORKs case has, MMCCYY, MMCCYY, This replaces your previous, Your Transitional CalFresh, Reporting, You are encouraged to report if, Recertification, and You will get a notice when it is.
It's very easy to make an error while filling out the Recertification, so you'll want to go through it again before you send it in.
3. This third part is normally easy - fill in all of the blanks in You may review them at your, CF REQUIRED FORM SUBSTITUTE, and Page of in order to complete the current step.

4. To move forward, your next part will require completing several form blanks. Included in these are cid, cid, If you ask your worker will get, OR Call toll free or for hearing, To Get Help You can ask about your, If you do not want to go to the, HEARING REQUEST, I want a hearing due to an action, n CalFresh n MediCal, You have the right to ask for a, If you ask for a hearing before an, Your Cash Aid or MediCal will stay, cid, cid, and If the hearing decision says we, which you'll find integral to going forward with this document.
5. This final step to finish this form is critical. Make sure you fill in the required fields, for instance Heres Why, n If you need more space check, n I need the state to provide me, A relative or friend cannot, My language or dialect is, NAME OF PERSON WHOSE BENEFITS WERE, BIRTH DATE, STREET ADDRESS, PHONE NUMBER, STATE, ZIP CODE, DATE, You may receive child care, If we told you your other, and If we told you we will pay your, before submitting. Or else, it might contribute to an incomplete and possibly incorrect paper!
Step 3: Always make sure that the details are correct and then click on "Done" to complete the task. Join FormsPal now and immediately gain access to 5-month, available for download. Each modification you make is handily preserved , helping you to modify the form at a later time if needed. We do not share the information you use while dealing with forms at FormsPal.