
Making use of the online PDF tool by FormsPal, you're able to complete or change dfas direct deposit authorization form right here and now. Our development team is continuously endeavoring to enhance the tool and help it become even faster for people with its extensive features. Enjoy an ever-improving experience now! If you're looking to begin, this is what it takes:
Step 1: Hit the "Get Form" button in the top part of this webpage to open our editor.
Step 2: Once you access the tool, you'll see the document all set to be completed. Apart from filling out different blanks, you can also perform many other actions with the file, that is writing custom textual content, editing the initial textual content, inserting illustrations or photos, signing the form, and more.
For you to complete this document, be certain to enter the right details in each blank field:
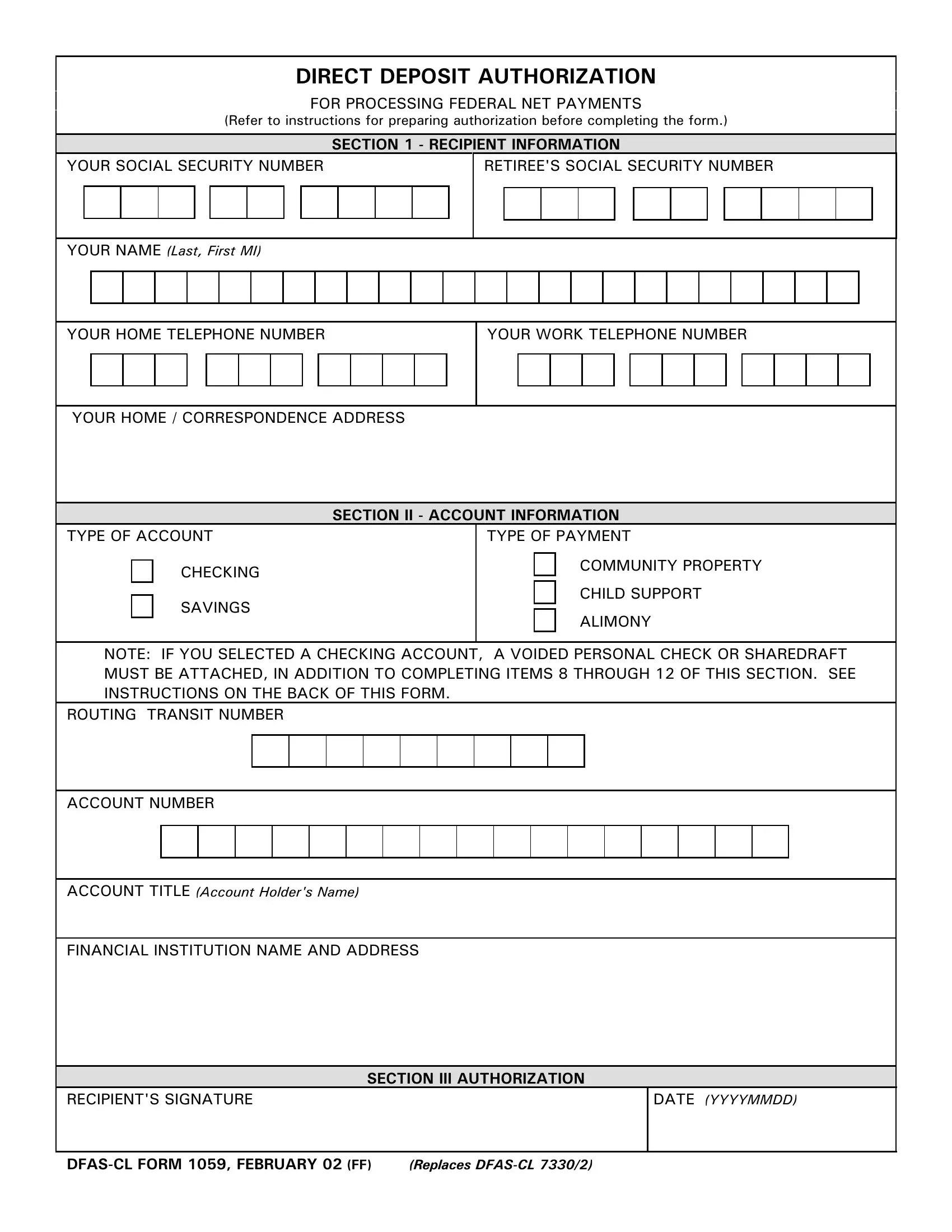
1. The dfas direct deposit authorization form will require specific details to be inserted. Be sure the next fields are finalized:
2. The subsequent part would be to fill in the next few fields: CHECKING, SAVINGS, TYPE OF PAYMENT, COMMUNITY PROPERTY, CHILD SUPPORT, ALIMONY, NOTE IF YOU SELECTED A CHECKING, ROUTING TRANSIT NUMBER, ACCOUNT NUMBER, ACCOUNT TITLE Account Holders Name, and FINANCIAL INSTITUTION NAME AND.
3. This next step is about RECIPIENTS SIGNATURE, DATE YYYYMMDD, and DFASCL FORM FEBRUARY FF Replaces - fill in all these blanks.

Always be extremely mindful when filling out DATE YYYYMMDD and RECIPIENTS SIGNATURE, since this is the part where a lot of people make errors.
Step 3: Soon after taking one more look at the form fields, press "Done" and you are done and dusted! Join FormsPal now and immediately obtain dfas direct deposit authorization form, all set for download. All alterations made by you are saved , so that you can edit the pdf at a later stage when required. Here at FormsPal.com, we do everything we can to be certain that your information is maintained private.