Dh Form 1960 is an important document for active duty service members and veterans. This form is used to request disability compensation from the Department of Veterans Affairs (VA). The VA examines each request and determines if the veteran meets the eligibility criteria for disability compensation. There are many factors that the VA considers when making a determination, so it is important to understand what is required on Dh Form 1960. This article will provide an overview of the form and explain the eligibility criteria. Additionally, we will highlight some of the benefits available to those who receive disability compensation from the VA.
| Question | Answer |
|---|---|
| Form Name | Dh Form 1960 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | false, birth certificate florida, 1960, REGISTRANT |
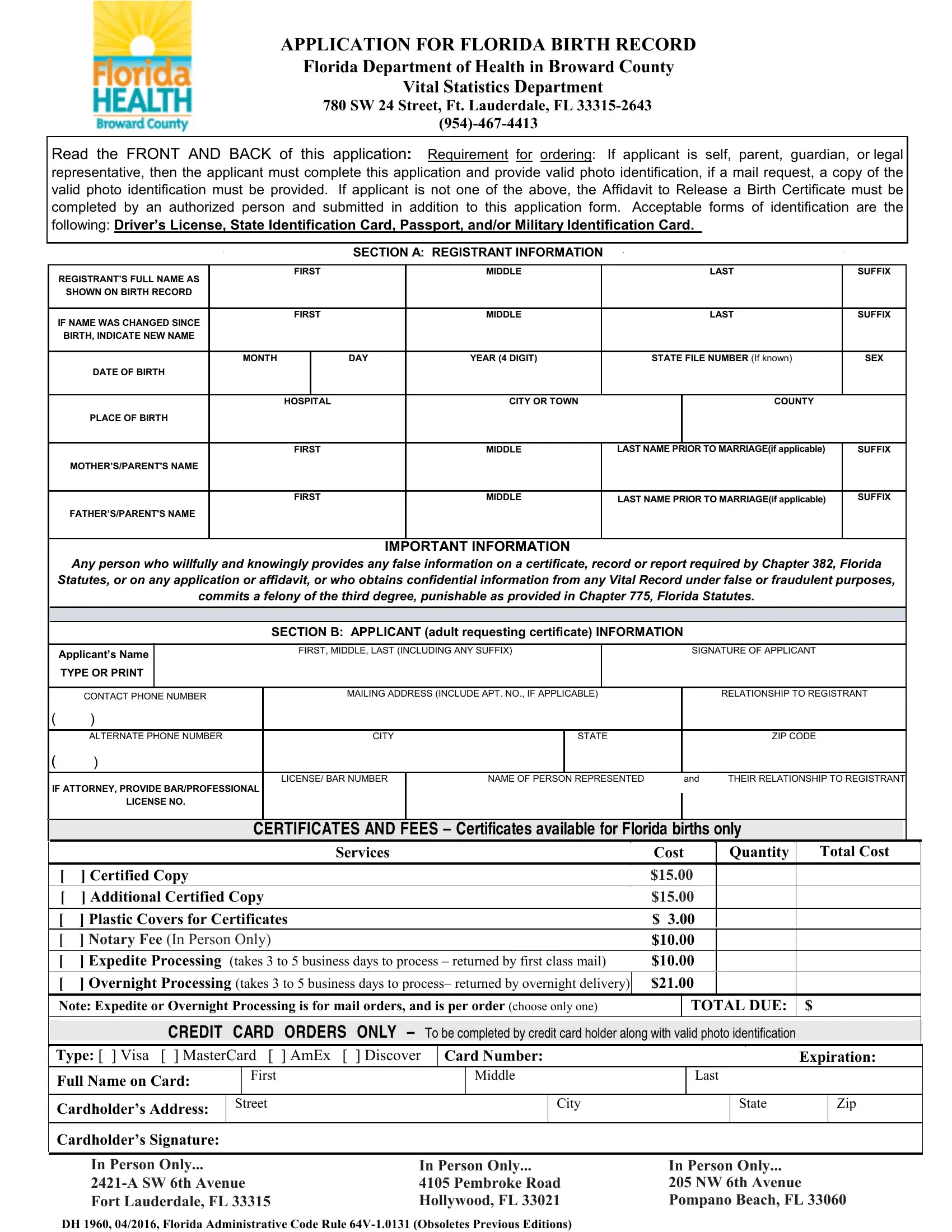
APPLICATION FOR FLORIDA BIRTH RECORD
Florida Department of Health in Broward County
Vital Statistics Department
780SW 24 Street, Ft. Lauderdale, FL
Requirement for ordering: If applicant is self, parent, guardian, or legal representative, then the applicant must complete this application and provide photo identification. If applicant is not one of the above, the Affidavit to Release A Birth Certificate must be completed by an authorized person and submitted in addition to this application form, along with photo identification. Acceptable forms of identification are the following: Driver’s
License, State Identification Card, Passport, and/or Military Identification Card.
PLEASE TYPE or PRINT ALL INFORMATION
(Registrant’s) |
|
|
FIRST |
|
|
|
MIDDLE |
|
|
|
LAST |
|
|
SUFFIX |
||
FULL NAME AT BIRTH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If name was changed since |
|
|
FIRST |
|
|
|
MIDDLE |
|
|
|
LAST |
|
|
SUFFIX |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
birth, indicate new name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLACE OF BIRTH |
|
|
HOSPITAL |
|
|
|
CITY |
|
|
|
COUNTY (REQUIRED) |
BIRTH FILE NUMBER |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(if known) |
||
FLORIDA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
MONTH |
|
DAY |
YEAR (4 DIGIT) |
|
IF YEAR IS NOT KNOWN ENTER |
|
|
NOT AVAILABLE |
|
|
AGE |
|
SEX |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
RANGE OF YEARS TO BE SEARCHED |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
LOCALLY |
|
|
|
|
|
|||
|
|
|
|
|
|
|
IN NEXT BOX |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MOTHER’S MAIDEN NAME |
|
|
FIRST |
|
|
|
MIDDLE |
|
|
|
LAST (MAIDEN) |
|
|
SUFFIX |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Name before marriage) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
FATHER’S NAME |
|
|
FIRST |
|
|
|
MIDDLE |
|
|
|
LAST |
|
|
SUFFIX |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(If the Father is listed) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IMPORTANT: READ THE ENTIRE APPLICATION BEFORE COMPLETING. |
|
|
|
||||||||||||
To obtain and use a Florida birth record under false or fraudulent purposes is a |
|
|
|
|||||||||||||
|
|
punishable by the terms and conditions set forth in Florida Statutes. |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CERTIFICATES AND FEES – Certificates available for Florida births only
|
|
|
|
|
|
|
|
|
|
|
Services |
Cost |
Quantity |
Total Cost |
||||||||||||||
|
|
[ |
] Certified Copy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$15.00 |
|
|
|
|
|
|||||
|
|
|
[ ] Optional Plastic Covers for Certificates |
|
|
|
|
|
|
|
|
|
$ |
3.00 |
|
|
|
|
|
|||||||||
|
|
|
[ ] Notary Fee (In Person Only) |
|
|
|
|
|
|
|
|
|
|
|
$ |
10.00 |
|
|
|
|
|
|||||||
|
|
[ |
] Expedite Processing (takes 3 to 5 business days to process – returned by first class mail) |
$10.00 |
|
|
|
|
|
|||||||||||||||||||
|
|
|
[ ] Overnight Processing (takes 3 to 5 business days to process– returned by overnight delivery) |
$21.00 |
|
|
|
|
|
|||||||||||||||||||
|
|
|
Note: Expedite or Overnight Processing is for mail orders, and is per order (choose only one) |
|
|
TOTAL DUE: |
$ |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
PLEASE READ ALL INFORMATION ON BACK BEFORE SUBMITTING APPLICATION |
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPLICANT’S NAME |
|
|
|
|
|
|
FIRST |
|
|
|
|
MIDDLE |
|
|
|
|
LAST |
|
SUFFIX |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
STATE RELATIONSHIP TO REGISTRANT |
|
SIGNATURE OF APPLICANT |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
HOME PHONE NUMBER |
|
|
|
|
RESIDENCE STREET ADDRESS (AND APT.) |
|
|
|
|
|
|
|
|
|||||||||||
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WORK PHONE NUMBER |
|
|
|
|
|
CITY |
|
|
STATE |
|
|
|
|
ZIP CODE |
||||||||||
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CREDIT CARD ORDERS ONLY – To be completed by credit card holder |
|
|
|
|
|
|||||||||||||
|
|
|
Type: [ ] Visa [ ] MasterCard [ ] AmEx [ |
] Discover |
Card Number: |
|
|
|
|
|
Expiration: |
|||||||||||||||||
|
|
|
Full Name on Card: |
|
First |
|
|
|
|
|
|
Middle |
|
|
Last |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Cardholder’s Address: |
|
Street |
|
|
|
|
|
|
|
City |
|
|
|
|
State |
|
Zip |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Cardholder’s Signature: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
OFFICIAL USE ONLY – To be completed by Florida Department of Health - Broward County staff |
||||||||||||||||||||
|
|
|
Date: |
|
|
|
Receipt #: |
|
|
|
|
|
|
Document #: |
|
|
|
|
|
|
|
|||||||
|
|
|
Driver’s License #: |
|
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
|
|
||||||||
|
|
|
In Person Only... |
|
|
|
|
|
In Person Only... |
|
|
|
|
In Person Only... |
||||||||||||||
|
|
|
2421A S.W. 6 Avenue |
|
|
|
|
|
4105 Pembroke Road |
|
|
|
|
205 NW 6th Avenue |
||||||||||||||
|
|
|
Ft. Lauderdale, FL 33315 |
|
|
|
|
|
Hollywood, FL 33021 |
|
|
|
|
Pompano Beach, FL 33060 |
||||||||||||||
DH Form 1960 (New 7/03) – Broward (08/01/03) - Revised 10/30/09
INFORMATION AND INSTRUCTIONS FOR BIRTH RECORD APPLICATION
AVAILABILITY:
State law did not require birth registration until the year 1917. However, there are some records on file at the State Office of Vital Statistics dating back to 1865. Most birth records between the years 1930 to present can be obtained through this office. Records on birth events that occurred in 1929 or earlier may be obtained from the State Office of Vital Statistics. Birth records under seal by reason of adoption, paternity determination or court order cannot be ordered in this manner. For a record under seal write to: State
Office of Vital Statistics, Attn: Records Amendment Section, Post Office Box 210, Jacksonville, Florida
ELIGIBILITY: |
|
|
Birth certificates can be issued only to: |
|
|
1) the registrant (the child named on the record) if of legal age (18) |
4) |
a legal representative of one of these persons, or |
2) parent |
5) |
by court order. |
3) guardian |
|
|
In the case of a deceased registrant, upon receipt of the death certificate of the decedent, certification of the birth certificate can be issued to the spouse, child, grandchild, sibling, if of legal age, or to the legal representative of any of these persons as well as to the parent.
Any person of legal age may be issued a certified copy of a birth record for a birth event that occurred over 100 years ago (except for those birth records under seal).
REQUIREMENT FOR ORDERING:
If applicant is self, parent, guardian, or legal representative the applicant must provide a completed application along with photo identification (ID). If guardian, a copy of an appointment order must be included. If legal representative, provide your attorney identification number (ID), and a notation of whom you are representing and their relationship to the registrant must be included with your request. If you are an agent of local, state or federal agency requesting a record, indicate in the space provided for “relationship” the name of the agency and that you are requesting for official purposes.
If not one of the above you will need to complete the form and have a notarized Affidavit to Release A Birth Certificate (DH Form 1958 2/03) submitted with your application for the birth record along with your photo identification.
RELATIONSHIP TO REGISTRANT:
A person ordering his or her own certificate should enter "SELF" in this space. Also, explain if name has been changed; married name, name changed legally (when and where), etc. Others must identify themselves clearly as eligible (see ELIGIBILITY above). If you are an agent of local, state or federal agency requesting a certificate, record for official purposes, indicate in the space provided for “relationship” the name of the agency and that you are requesting the certificate for official purposes.
APPLICANT’S SIGNATURE:
Applicant’s signature is required, as well as his/her printed name, residence address and a valid telephone number.
ACCEPTABLE FORMS OF IDENTIFICATION:
Driver’s License, State Identification Card, Passport, and/or Military Identification Card.
PAYMENT: Cash, Credit Cards, Money Orders, Cashier’s Checks or Bank Drafts; Personal Checks accepted only from Broward,
Make payable to: Florida Department of Health in Broward County
ADDRESS ON CHECK AND PHOTO IDENTIFICATION MUST BE THE SAME
MAIL ORDERS: Regular mail orders must include a
Mail to: Florida Department of Health - Broward County Vital Statistics Department, 780 S.W. 24th Street, Ft. Lauderdale, FL
PHONE or INTERNET ORDERS: Requires the use of a credit card. Requires Expedite and either Regular or Overnight Processing. Must include a copy of an acceptable form of Identification; Phone (866)
DH Form 1960 (New 7/03) – Broward (08/01/03) - Revised 10/30/09