
In case you desire to fill out dhcs 6168 third party liability notification in spanish, you don't have to install any kind of software - simply try our online PDF editor. To maintain our tool on the cutting edge of practicality, we work to put into action user-driven features and improvements regularly. We are always grateful for any suggestions - play a vital role in reshaping PDF editing. All it requires is a few basic steps:
Step 1: Just click on the "Get Form Button" at the top of this page to access our form editor. Here you will find everything that is required to work with your document.
Step 2: The tool helps you work with nearly all PDF documents in various ways. Change it by adding any text, correct original content, and add a signature - all within several mouse clicks!
If you want to fill out this form, make sure you provide the right information in each blank:
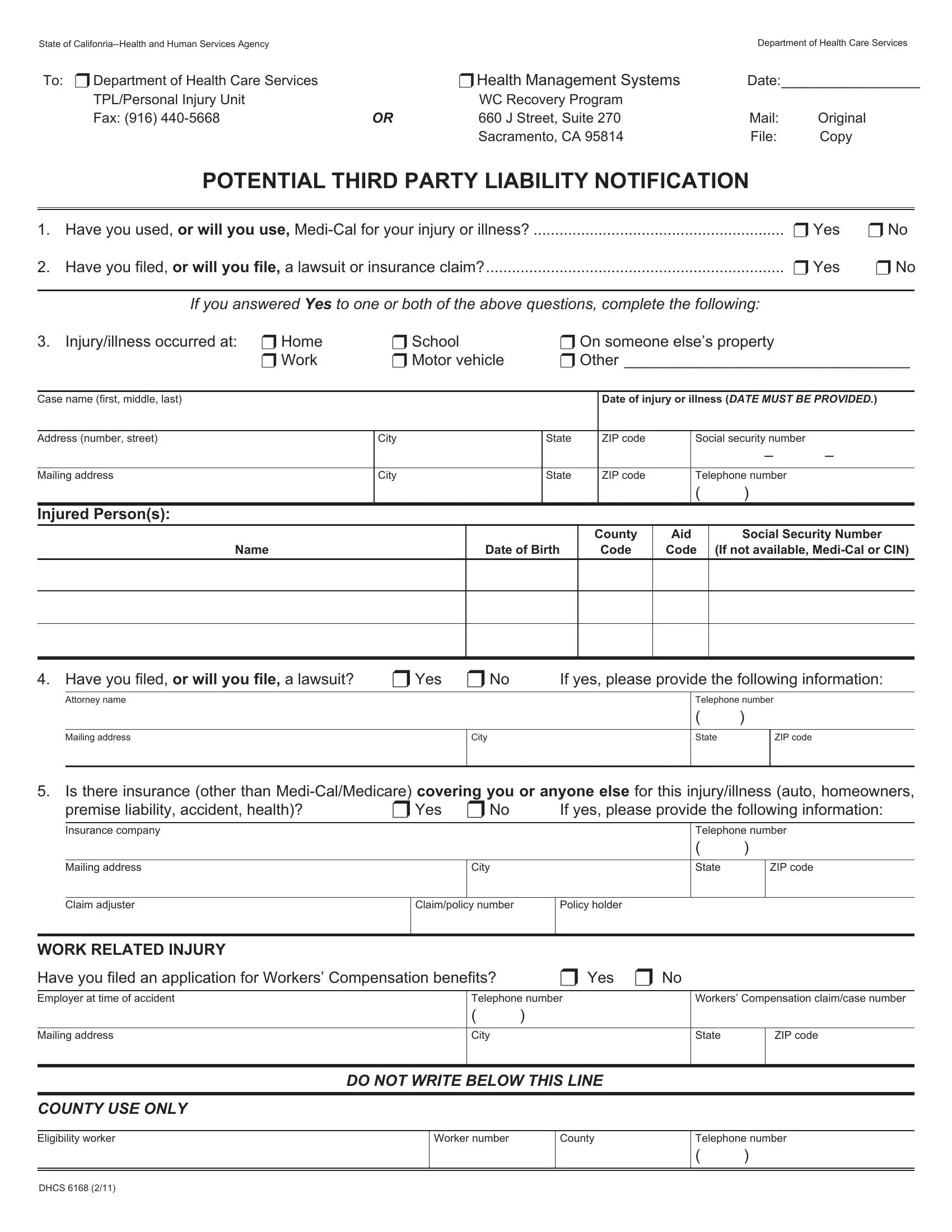
1. The dhcs 6168 third party liability notification in spanish usually requires certain details to be inserted. Make sure the subsequent blank fields are complete:
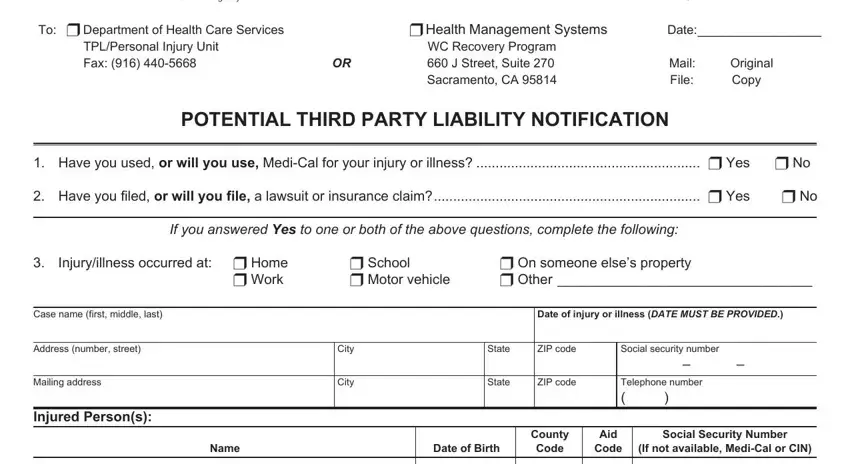
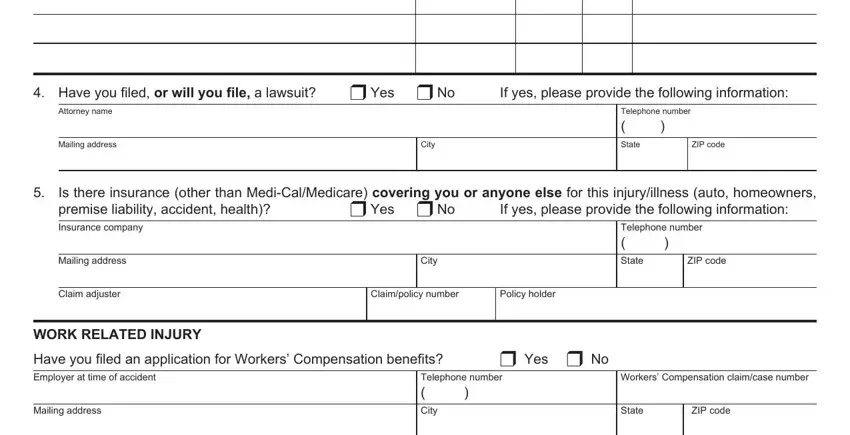
2. Once your current task is complete, take the next step – fill out all of these fields - Have you filed or will you file a, u No, If yes please provide the, Attorney name, Mailing address, City, State, ZIP code, Telephone number, Is there insurance other than, u Yes u No, covering you or anyone else for, If yes please provide the, Insurance company, and Mailing address with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It is possible to make a mistake while filling in the State, and so be sure you look again prior to deciding to send it in.
Step 3: Before finalizing your document, you should make sure that form fields were filled in as intended. The moment you think it is all good, click on “Done." Right after registering afree trial account with us, you will be able to download dhcs 6168 third party liability notification in spanish or send it via email right away. The PDF will also be available from your personal account with all your adjustments. We do not share or sell the information that you provide while dealing with forms at FormsPal.