
Working with PDF forms online can be super easy with this PDF editor. Anyone can fill out dhcs 6247 here painlessly. The editor is continually improved by our team, acquiring useful features and becoming more convenient. With some simple steps, you are able to start your PDF editing:
Step 1: First, open the pdf editor by clicking the "Get Form Button" at the top of this webpage.
Step 2: The editor provides the capability to change PDF forms in many different ways. Transform it by writing your own text, adjust what's already in the PDF, and include a signature - all at your convenience!
To be able to complete this document, be sure you type in the right information in each and every blank:
1. You should fill out the dhcs 6247 properly, thus take care when working with the sections including all of these blanks:
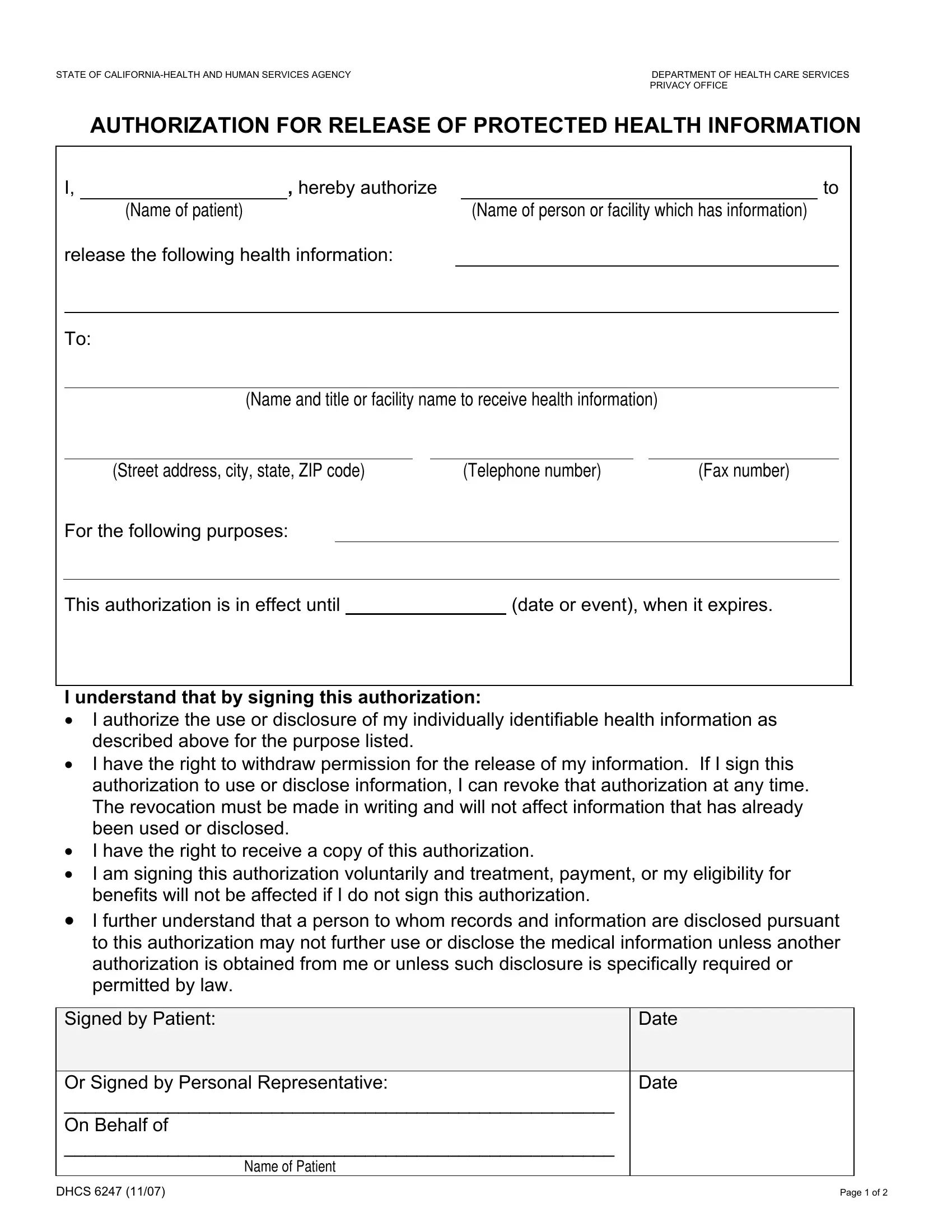
2. The subsequent part is to fill out these blank fields: For the following purposes, This authorization is in effect, date or event when it expires, I understand that by signing this, I authorize the use or disclosure, I further understand that a, Signed by Patient, and Date.
3. This next segment will be about Or Signed by Personal, Date, DHCS, and Page of - type in each of these blanks.

4. The fourth subsection comes with the next few blank fields to focus on: COPY OF IDENTIFICATION ATTACHED, TYPE IDENTIFICATION CARD BIRTH, CA DRIVERS LICENSE CA DMV, NUMBER, IF NO IDENTIFICATION IS ATTACHED, NOTARIZED, NOTARIZED BY, DATE, and NOTARY PUBLIC NUMBER.
Be extremely mindful while completing TYPE IDENTIFICATION CARD BIRTH and NUMBER, as this is where many people make mistakes.
5. The pdf should be concluded by going through this area. Here there can be found a comprehensive list of form fields that need accurate details for your form usage to be faultless: PARENT, GUARDIAN, CONSERVATOR, EXECUTOR OF WILL, MEDICAL POWER OF ATTORNEY, OTHER, NOTE ATTACHING LEGAL DOCUMENTATION, DHCS, and Page of.
Step 3: After looking through your entries, click "Done" and you are all set! Join FormsPal now and easily gain access to dhcs 6247, prepared for downloading. Each and every change you make is handily kept , which enables you to modify the document later on anytime. FormsPal guarantees your data privacy by using a protected system that never saves or distributes any sort of personal data involved in the process. Be confident knowing your docs are kept confidential any time you work with our tools!