
It is possible to prepare Guamanian effectively with our PDFinity® editor. FormsPal team is devoted to providing you with the best possible experience with our editor by continuously introducing new features and enhancements. With all of these updates, working with our tool becomes better than ever before! With just a few simple steps, you are able to start your PDF editing:
Step 1: Click the orange "Get Form" button above. It'll open our pdf editor so you could begin completing your form.
Step 2: This editor enables you to work with PDF files in many different ways. Enhance it by writing any text, correct original content, and add a signature - all at your convenience!
This document will need particular information to be entered, therefore make sure you take the time to type in what's expected:
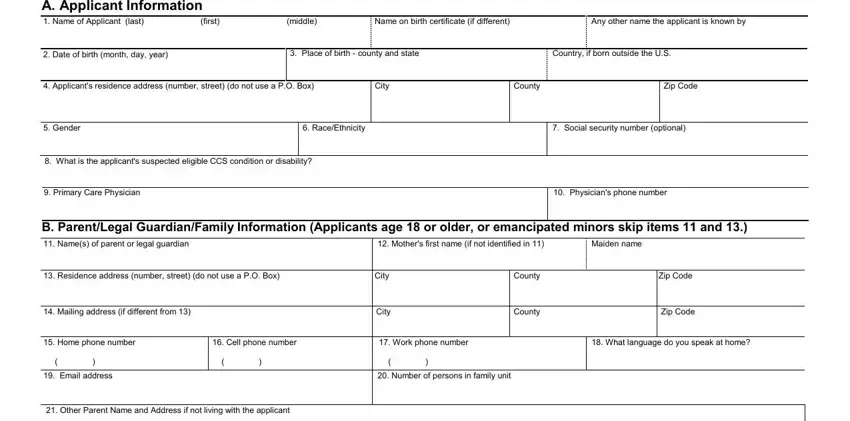
1. First of all, once completing the Guamanian, begin with the area with the next blanks:
2. Just after finishing the last section, head on to the next stage and complete all required details in all these blank fields - C Health Insurance Information, If yes what is the applicants, Yes, nnumber, a Does the applicant have other, Type of insurance plan or company, Is there a shareofcost No, Yes, If yes what is the amount you pay, b If yes what is the name of the, company, c Policy or Plan Number, Preferred Provider Organization PPO, Health Maintenance Organization, and Does the applicant have dental.
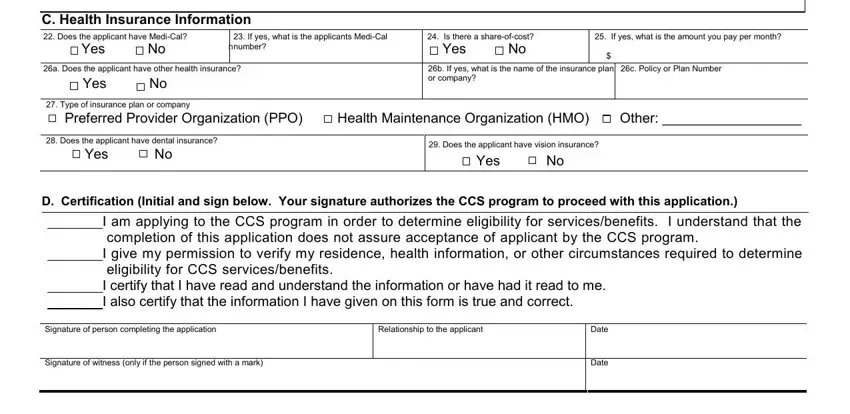
As for nnumber and c Policy or Plan Number, make sure you get them right in this current part. Both of these are certainly the most important ones in this page.
Step 3: Revise everything you've typed into the blank fields and click the "Done" button. Join FormsPal today and easily gain access to Guamanian, ready for downloading. Each edit you make is conveniently saved , which means you can customize the document at a later time if required. FormsPal ensures your data confidentiality by using a secure system that in no way saves or shares any type of personal information provided. Rest assured knowing your docs are kept confidential every time you use our services!