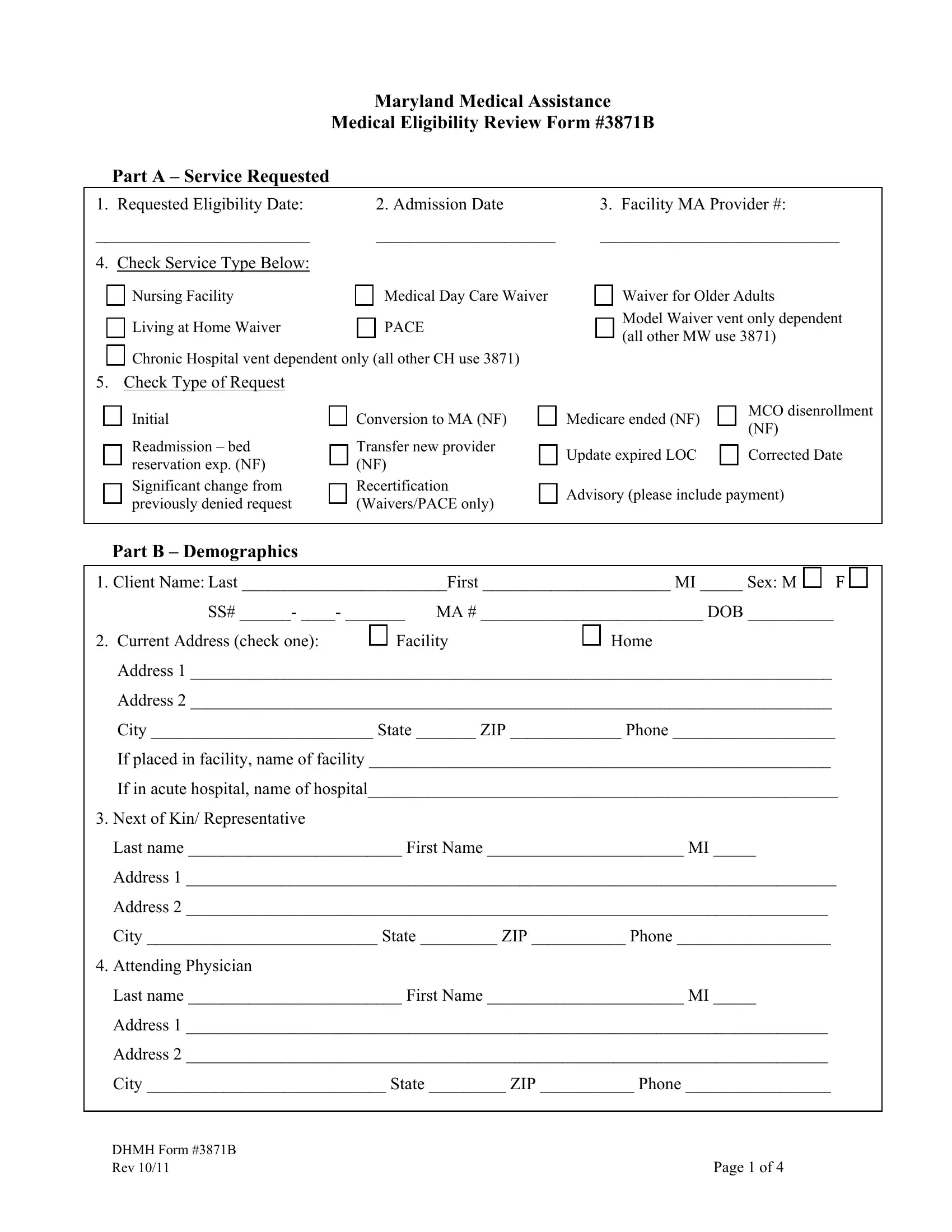
Maryland Medical Assistance
Medical Eligibility Review Form #3871B
Part A – Service Requested
1. Requested Eligibility Date: |
|
|
|
2. Admission Date |
|
3. Facility MA Provider #: |
_________________________ |
|
|
|
|
_____________________ |
____________________________ |
4. Check Service Type Below: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nursing Facility |
|
|
|
Medical Day Care Waiver |
|
|
Waiver for Older Adults |
|
|
|
|
|
|
|
|
|
|
|
|
|
Living at Home Waiver |
|
|
|
PACE |
|
|
Model Waiver vent only dependent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(all other MW use 3871) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chronic Hospital vent dependent only (all other CH use 3871) |
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Check Type of Request |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initial |
|
|
|
|
Conversion to MA (NF) |
|
|
Medicare ended (NF) |
|
|
|
MCO disenrollment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(NF) |
|
|
|
|
Readmission – bed |
|
|
|
Transfer new provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Update expired LOC |
|
|
|
Corrected Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
reservation exp. (NF) |
|
|
|
(NF) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Significant change from |
|
|
Recertification |
|
Advisory (please include payment) |
|
|
|
|
|
|
|
|
|
|
previously denied request |
|
|
|
|
(Waivers/PACE only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part B – Demographics
|
|
|
|
|
|
|
|
|
1. Client Name: Last ________________________First ______________________ MI _____ Sex: M |
|
|
F |
SS# ______- ____- _______ |
MA # __________________________ DOB __________ |
|
2. Current Address (check one): |
|
Facility |
|
Home |
|
|
|
|
|
|
|
Address 1 ___________________________________________________________________________
Address 2 ___________________________________________________________________________
City __________________________ State _______ ZIP _____________ Phone ___________________
If placed in facility, name of facility ______________________________________________________
If in acute hospital, name of hospital_______________________________________________________
3.Next of Kin/ Representative
Last name _________________________ First Name _______________________ MI _____
Address 1 ____________________________________________________________________________
Address 2 ___________________________________________________________________________
City ___________________________ State _________ ZIP ___________ Phone __________________
4.Attending Physician
Last name _________________________ First Name _______________________ MI _____
Address 1 ___________________________________________________________________________
Address 2 ___________________________________________________________________________
City ____________________________ State _________ ZIP ___________ Phone _________________
DHMH Form #3871B |
|
Rev 10/11 |
Page 1 of 4 |
Applicant Name ____________________________
Part C – MR/MI Please Complete the Following on All Individuals:
|
|
|
|
|
|
|
|
|
Review Item |
|
|
|
|
|
Answer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
|
N |
1. |
Is there a diagnosis or presenting evidence of mental retardation/related condition, or has the client received |
|
|
|
|
|
|
|
|
|
|
|
|
|
MR services within the past two years? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Is there any presenting evidence of mental illness? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please note: Dementia/Alzheimer’s is not considered a mental illness. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. If yes, check all that apply. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Schizophrenia |
|
|
|
Personality disorder |
|
|
Somatoform disorder |
|
Panic or severe anxiety disorder |
|
|
|
|
|
|
|
|
|
|
|
|
Mood disorder |
|
|
Paranoia |
|
|
Other psychotic or mental disorder leading to chronic disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Has the client received inpatient services for mental illness within the past two years? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Is the client on any medication for the treatment of a major mental illness or psychiatric diagnosis? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. If yes, is the mental illness or psychiatric diagnosis controlled with medication? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Is the client a danger to self or others? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part D – Diagnoses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary diagnosis related to the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
need for requested level of care |
|
ICD Code |
|
|
Description |
|
|
|
|
|
|
Other active diagnoses related to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the need for requested level of care |
|
Descriptions |
|
|
|
|
|
|
|
|
|
|
|
Part E – Skilled Services:
Requires a physician’s order. Requires the skills of technical or professional personnel such as a registered nurse, licensed practical nurse, respiratory therapist, physical therapist, and/or occupational therapist. The service must be inherently complex such that it can be safely and effectively performed only by, or under the supervision of, professional or technical personnel. Items listed under Rehabilitation and Extensive Services may overlap.
Table I. Extensive Services (serious/unstable medical condition and need for service)
|
Review Item |
|
# of days service is |
|
(Please indicate the number of days per week each service is required) |
|
required/wk. (0-7) |
|
|
|
1. |
Tracheotomy Care: All or part of the day |
|
|
|
|
|
|
2. |
Suctioning: Not including routine oral-pharyngeal suctioning, at least once a day |
|
|
|
|
|
|
3. |
IV Therapy: Peripheral or central (not including self-administration) |
|
|
|
|
|
|
4. |
IM/SC Injections: At least once a day (not including self-administration) |
|
|
|
|
|
|
5. |
Pressure Ulcer Care: Stage 3 or 4 and one or more skin treatments (including pressure- |
|
|
relieving bed, nutrition or hydration intervention, application of dressing and/or medications) |
|
|
|
|
6. Wound Care: Surgical wounds or open lesions with one or more skin treatments per day (e.g., |
|
application of a dressing and/or medications daily) |
|
|
|
|
|
|
7. |
Tube Feedings: 51% or more of total calories or 500 cc or more per day fluid intake via tube |
|
|
8. |
Ventilator Care: Individual would be on a ventilator all or part of the day |
|
|
|
|
|
|
9. |
Complex respiratory services: Excluding aerosol therapy, spirometry, postural drainage or |
|
|
routine continuous O2 usage |
|
|
|
|
|
10. Parenteral Feeding or TPN: Necessary for providing main source of nutrition. |
|
|
|
|
|
11. Catheter Care: Not routine foley |
|
|
|
|
|
12. Ostomy Care: New |
|
|
|
|
|
DHMH Form #3871B |
|
|
Rev 10/11 |
Page 2 of 4 |
Applicant Name ____________________________
13.Monitor Machine: For example, apnea or bradycardia
14.Formal Teaching/Training Program: Teach client or caregiver how to manage the treatment regime or perform self care or treatment skills for recently diagnosed conditions (must be ordered by a physician)
Table II. Rehabilitation (PT/OT/Speech Therapy services) Must be current ongoing treatment.
Review Item |
No. of days service |
(Please indicate the number of days per week each service is required. |
is required/wk. |
|
(0-7) |
15.Extensive Training for ADLs. (restoration, not maintenance), including walking, transferring, swallowing, eating, dressing and grooming.
16.Amputation/Prosthesis Care Training: For new amputation.
17.Communication Training: For new diagnosis affecting ability to communicate.
18.Bowel and/or Bladder Retraining Program: Not including routine toileting schedule.
Part F – Functional Assessment
Review Item |
Answer |
Cognitive Status (Please answer Yes or No for EACH item.) |
Y |
|
N |
1. Orientation to Person: Client is able to state his/her name. |
|
|
|
|
2.Medication Management: Able to administer the correct medication in the correct dosage, at the correct frequency without the assistance or supervision of another person.
3.Telephone Utilization: Able to acquire telephone numbers, place calls, and receive calls without the assistance or supervision of another person.
4.Money Management: Can manage banking activity, bill paying, writing checks, handling cash transactions, and making change without the assistance or supervision of another person.
5.Housekeeping: Can perform the minimum of washing dishes, making bed, dusting, and laundry, straightening up without the assistance or supervision of another person.
6. Brief Interview for Mental Status (BIMS): Was the examiner able to administer the complete interview? If yes, indicate the final score. If no, indicate reason.
|
If yes, Score: ____________ |
(Examination should be administered in a language in which the client is fluent.) |
If No, check one of the following: |
|
|
|
|
|
|
|
|
Hearing Loss |
|
|
|
|
|
Applicant is rarely/never understood |
|
|
|
|
|
|
|
|
Language Barrier |
|
|
|
Refused |
|
|
|
|
|
|
|
Other |
|
|
|
|
(specify) ______________________ |
Behavior (Please answer Yes or No for EACH item.) |
Answer |
|
Y N |
7.Wanders (several times a day): Moves with no rational purpose or orientation, seemingly oblivious to needs or safety.
8.Hallucinations or Delusions (at least weekly): Seeing or hearing nonexistent objects or people, or a persistent false psychotic belief regarding the self, people, or objects outside of self.
9.Aggressive/abusive behavior (several times a week): Physical and verbal attacks on others including
but not limited to threatening others, hitting, shoving , scratching, punching, pushing, biting, pulling hair or destroying property.
10.Disruptive/socially inappropriate behavior (several times a week): Interferes with activities of others or own activities through behaviors including but not limited to making disruptive sounds, self- abusive acts, inappropriate sexual behavior, disrobing in public, smearing/throwing food/feces, hoarding, rummaging through other’s belongings, constantly demanding attention, urinating in inappropriate places.
11.Self-injurious behavior (several times a month): Repeated behaviors that cause injury to self, biting, scratching, picking behaviors, putting inappropriate object into any body cavity, (including ear, mouth, or nose), head slapping or banging.
DHMH Form #3871B |
|
Rev 10/11 |
Page 3 of 4 |
Applicant Name ____________________________
|
|
Answer |
Communication (Please answer Yes or No for EACH item.) |
|
Y |
|
N |
12. Hearing Impaired even with use of hearing aid: Difficulty hearing when not in quiet setting, |
|
|
|
|
|
understands conversations only when face to face (lip-reading), can hear only very loud voice or totally |
|
|
|
|
|
deaf. |
|
|
|
|
|
13.Vision Impaired even with correction: Difficulty with focus at close range, field of vision is severely limited (tunnel vision or central vision loss), only sees light, motion, colors or shapes, or is totally blind.
14.Self Expression: Unable to express information and make self understood using any means (with the exception of language barrier).
Review Item
FUNCTIONAL STATUS: Score as Follows |
|
0 |
= Independent: No assistance or oversight required |
|
1 |
= Supervision: Verbal cueing, oversight, encouragement |
|
2 |
= Limited assistance: Requires hands on physical assistance |
Score Each Item |
3 |
= Extensive assistance: Requires full performance (physical assistance and verbal cueing) by |
(0-4) |
another for more than half of the activity. |
|
4 |
= Total care: Full activity done by another |
|
15.Mobility: Purposeful mobility with or without assistive devices.
16.Transferring: The act of getting in and out of bed, chair, or wheelchair. Also, transferring to and from toileting, tub and/or shower.
17.Bathing (or showering): Running the water, washing and drying all parts of the body, including hair and face.
18.Dressing: The act of laying out clothes, putting on and removing clothing, fastening of clothing and footwear, includes prostheses, orthotics, belts, pullovers.
19.Eating: The process of putting foods and fluids into the digestive system (including tube feeding).
20.Toileting: Ability to care for body functions involving bowel and bladder activity, adjusting clothes, wiping, flushing of waste, use of bedpan or urinal, and management of any special devices (ostomy or catheter). This does not include transferring (See transferring item 16 above).
CONTINENCE STATUS: Score as Follows
0 = Independent: Totally continent, can request assistance in advance of need, accidents only once or twice a week or is able to completely care for ostomy.
1 = Dependent: Totally incontinent, accidents three or more times a week, unable to request |
Score Each Item |
assistance in advance of need, continence maintained on toileting schedule, indwelling, suprapubic |
(0-1) |
or Texas catheter in use or unable to care for own ostomy. |
|
21.Bladder Continence: Ability to voluntarily control the release of urine from the bladder
22.Bowel Continence: Ability to voluntarily control the discharge of stool from the bowel.
Part G – Certification
1.Signature of Person Completing Form: _____________________________________ Date________________
Printed Name________________________________________
I certify to the best of my knowledge the information on the form is correct.
2.Signature of Health Care Professional: ______________________________________ Date________________
Printed Name_______________________________________
DHMH Form #3871B |
|
Rev 10/11 |
Page 4 of 4 |