
You are able to fill out dhs department ser instantly in our online PDF editor. To retain our tool on the cutting edge of efficiency, we strive to implement user-driven capabilities and enhancements regularly. We're always looking for suggestions - play a vital role in remolding PDF editing. By taking a couple of simple steps, you may begin your PDF journey:
Step 1: First, open the tool by clicking the "Get Form Button" in the top section of this webpage.
Step 2: With our online PDF editor, you'll be able to accomplish more than simply complete forms. Express yourself and make your forms look sublime with custom text incorporated, or modify the file's original input to excellence - all supported by the capability to add any type of pictures and sign the file off.
It will be easy to complete the form with our practical tutorial! Here's what you should do:
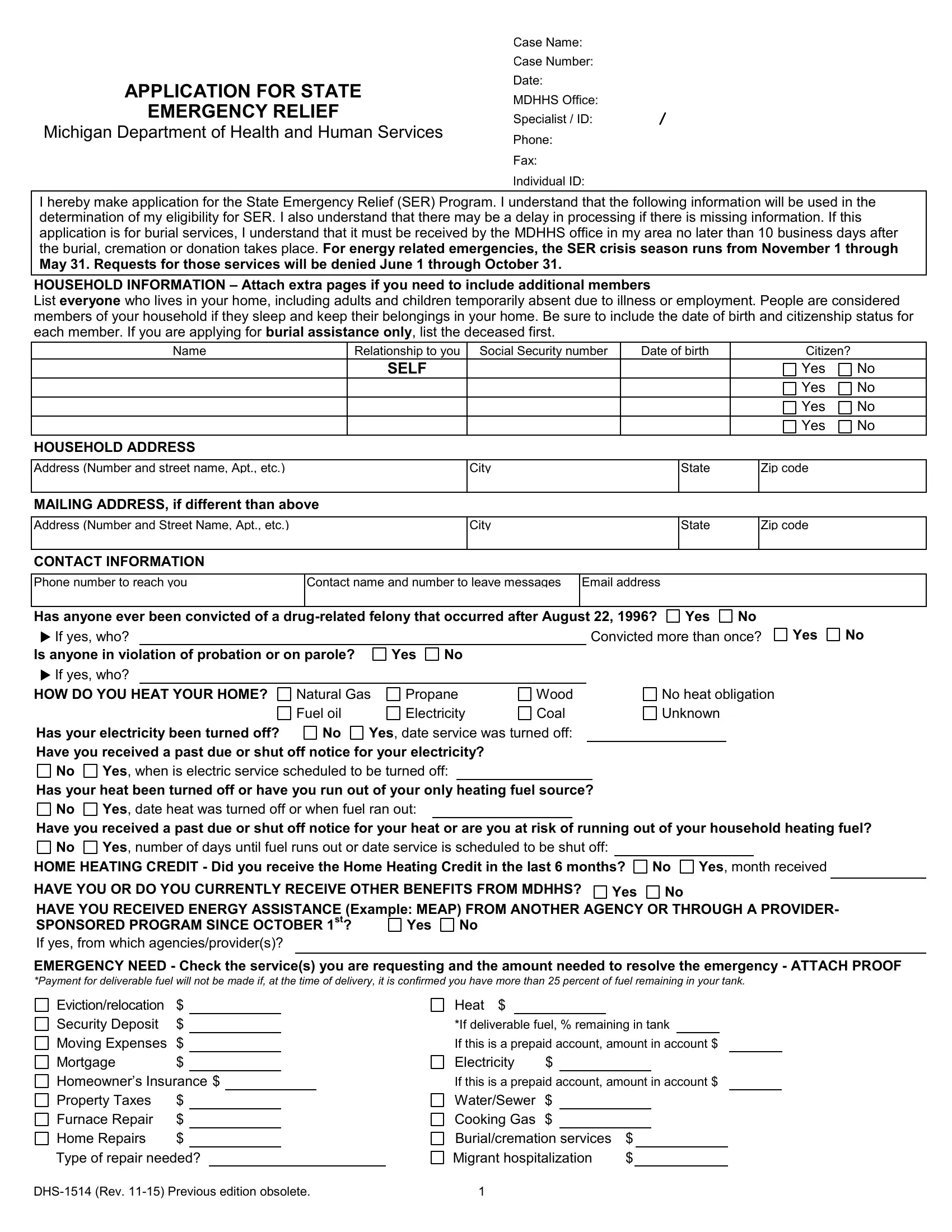
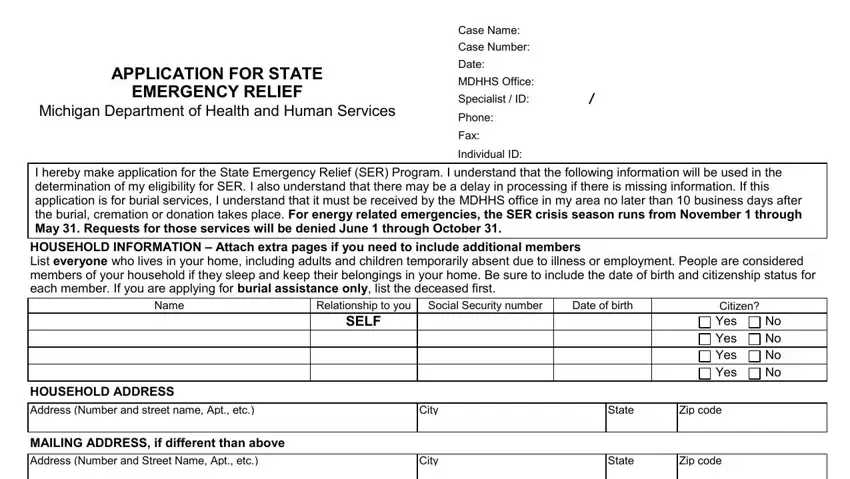
1. Begin filling out the dhs department ser with a selection of essential fields. Consider all of the important information and make sure not a single thing forgotten!
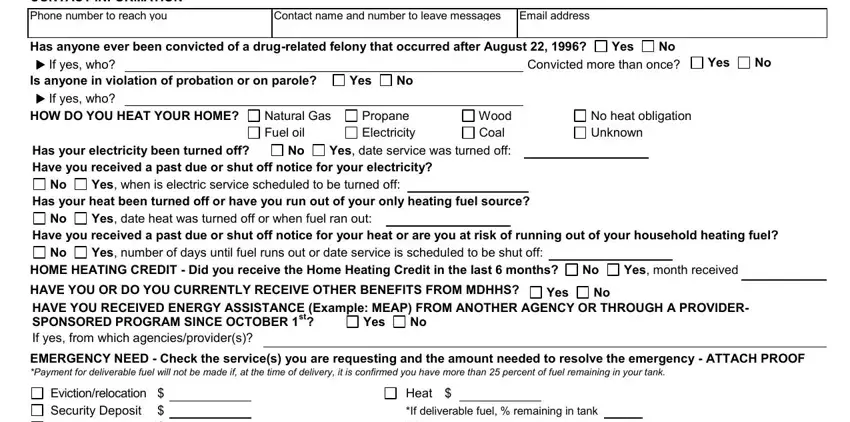
2. Once your current task is complete, take the next step – fill out all of these fields - CONTACT INFORMATION, Phone number to reach you, Contact name and number to leave, Email address, Has anyone ever been convicted of, Natural Gas Fuel oil No, Yes date service was turned off, Propane Electricity, Wood Coal, Yes, Has your heat been turned off or, Yes when is electric service, No Convicted more than once, Yes, and Yes with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
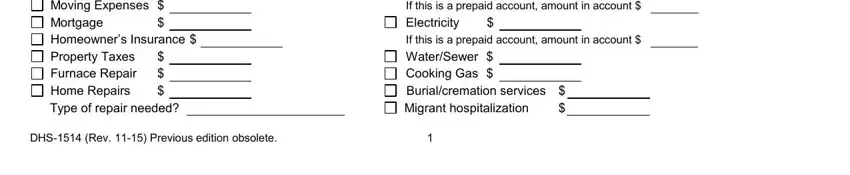
3. Your next part is usually straightforward - fill out all of the empty fields in Evictionrelocation Security, If deliverable fuel remaining in, Electricity, If this is a prepaid account, WaterSewer Cooking Gas, and DHS Rev Previous edition obsolete to complete this part.
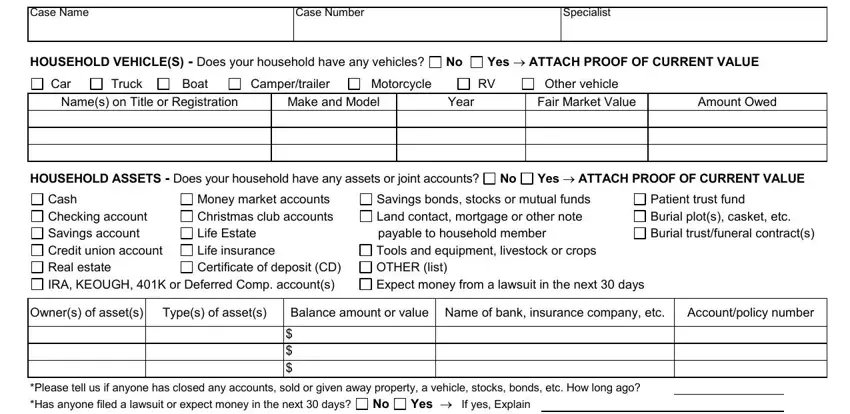
4. To go onward, your next form section will require filling out several blanks. Included in these are Case Name, Case Number, Specialist, HOUSEHOLD VEHICLES Does your, Campertrailer, Truck, Boat, Car, Names on Title or Registration, Make and Model, Year, Yes ATTACH PROOF OF CURRENT VALUE, Other vehicle Fair Market Value, Amount Owed, and HOUSEHOLD ASSETS Does your, which you'll find crucial to continuing with this particular PDF.
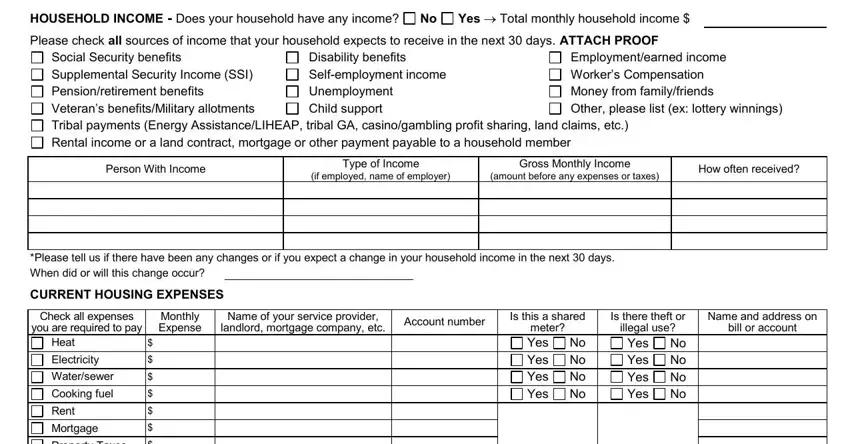
5. The very last point to finalize this PDF form is crucial. Make sure to fill out the required fields, for instance HOUSEHOLD INCOME Does your, Yes Total monthly household, Social Security benefits, Disability benefits Selfemployment, Employmentearned income Workers, Person With Income, Type of Income, Gross Monthly Income, if employed name of employer, amount before any expenses or taxes, How often received, Please tell us if there have been, Is this a shared, Is there theft or, and Name and address on, before using the pdf. Failing to do so might generate an unfinished and probably unacceptable paper!
As for How often received and if employed name of employer, ensure that you double-check them in this section. Both these are the most important fields in this file.
Step 3: Before obtaining the next step, make sure that all blank fields have been filled in the correct way. When you believe it is all good, click on “Done." Find the dhs department ser as soon as you join for a free trial. Instantly view the pdf from your personal cabinet, along with any modifications and changes all saved! When you work with FormsPal, you can easily complete forms without stressing about personal data leaks or entries getting distributed. Our secure system makes sure that your personal information is kept safely.