The PDF editor makes managing files trouble-free. It is extremely not hard to modify the [FORMNAME] file. Follow the following actions if you need to achieve this:
Step 1: To get going, hit the orange button "Get Form Now".
Step 2: As soon as you have accessed the dhs request michigan form edit page, you'll discover all functions you can undertake with regards to your document in the upper menu.
These parts are what you will need to fill out to get the ready PDF file.
Provide the requested particulars in the segment REQUEST FOR HEARING INSTRUCTIONS, Date Received in MDHHS, Programs in Dispute, If you do not agree with any, Someone else may represent you at, To Ask for a Hearing A request for, Appointment of an Authorized, Your Hearing Request will be, and We receive your request more than.
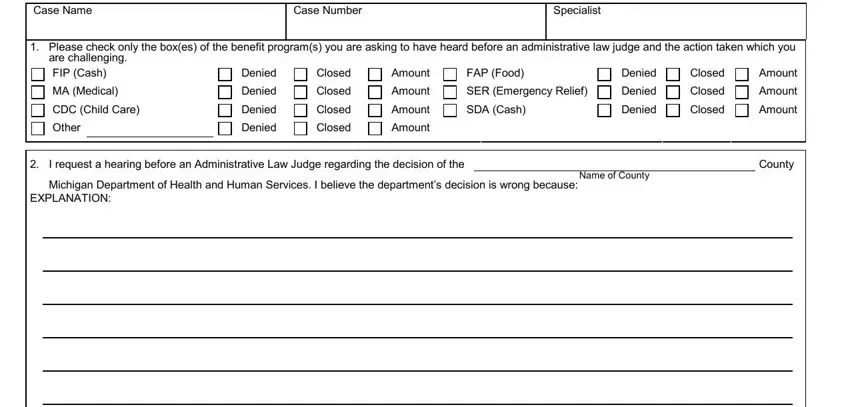
It is essential to put down certain details within the segment Case Name, Case Number, Specialist, Please check only the boxes of, are challenging FIP Cash MA, Denied Denied Denied Denied, Closed Closed Closed Closed, Amount Amount Amount Amount, FAP Food SER Emergency Relief SDA, Denied Denied Denied, Closed Closed Closed, Amount Amount Amount, I request a hearing before an, County, and Michigan Department of Health and.
You'll have to describe the rights and obligations of each party in box If necessary for participation at, Please identify the disability or, If at the hearing you are denied, By signing this form I acknowledge, I Signature of Person Requesting, and DO NOT want to continue receiving.
Review the fields I Signature of Person Requesting, Telephone Number, Date, Street Address or Route Number, Case Number, City State and Zip Code, THIS SECTION TO BE COMPLETED ONLY, Telephone Number, Title, Street Address or Route Number, City State and Zip Code, El Michigan Department of Health, and DHS Rev Previous edition obsolete and next complete them.
Step 3: Select the Done button to save the file. At this point it is accessible for transfer to your gadget.
Step 4: You may create duplicates of the form tostay clear of any kind of possible difficulties. You need not worry, we do not disclose or check your data.
