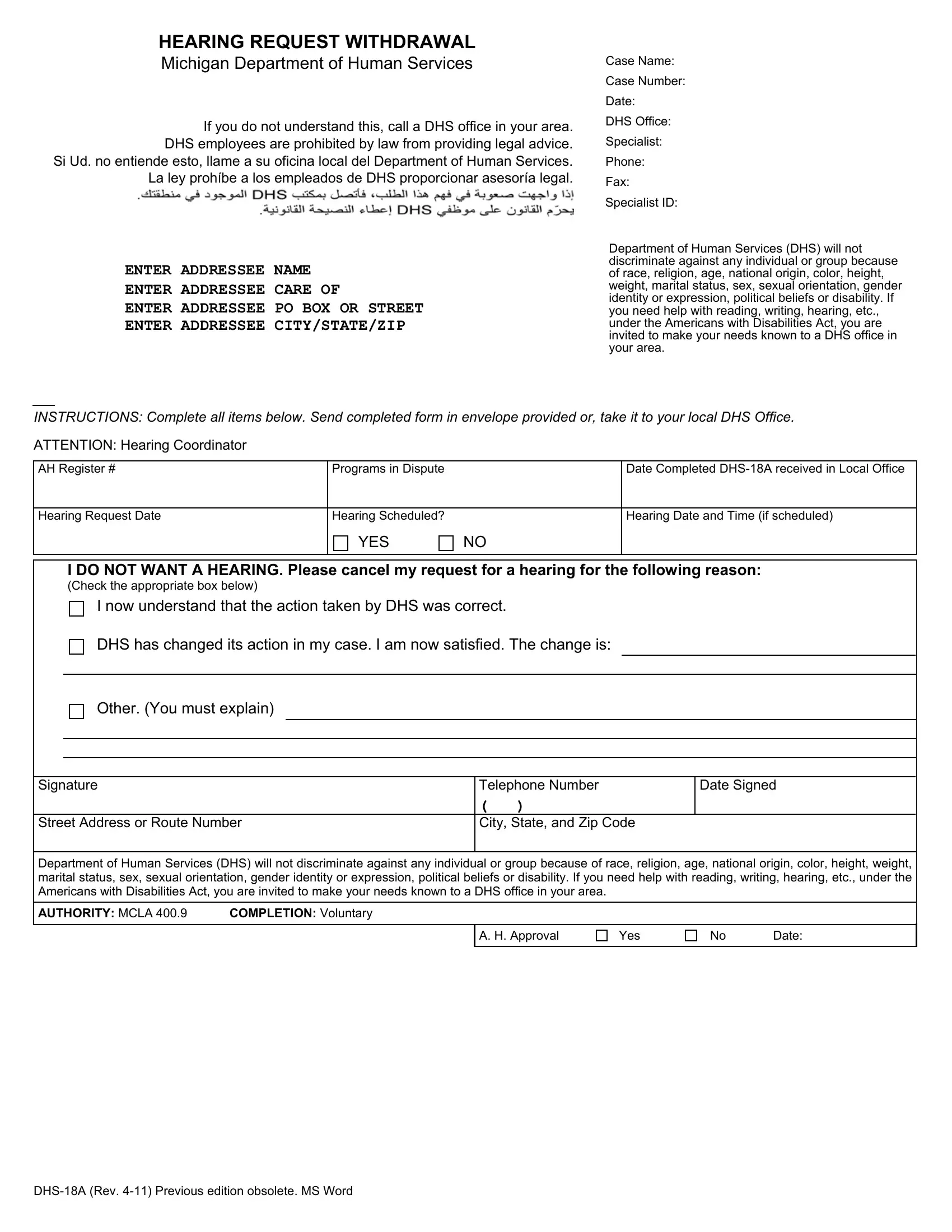
Navigating the paperwork involved with government services can sometimes feel overwhelming. The DHS 18A form serves as a critical document for individuals looking to withdraw their request for a hearing with the Michigan Department of Human Services. This form is especially relevant when a person initially believed they needed to challenge a decision made by the DHS but later decided against it for reasons such as understanding the correctness of the action taken by DHS, or because the department has made satisfactory changes to their case. The form clearly outlines the necessary fields one must complete, including personal information and specific details about the case and the hearing. It also emphasizes the importance of non-discrimination and accessibility, assuring that the DHS upholds values of equality and support for individuals regardless of race, religion, age, and other identifiers, while also providing accommodations as mandated by the Americans with Disabilities Act. Completion of the form is voluntary, but it is a vital step for those who choose to navigate their circumstances with the DHS. Moreover, instructions are provided to guide individuals on where to send or take the completed form, making the process as straightforward as possible.
| Question | Answer |
|---|---|
| Form Name | Dhs 18A Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DHS 0018 A_162674_7 dhs michigan hearing request withdrawal what is ah register # form |
HEARING REQUEST WITHDRAWAL
Michigan Department of Human Services
Case Name:
If you do not understand this, call a DHS office in your area. DHS employees are prohibited by law from providing legal advice.
Si Ud. no entiende esto, llame a su oficina local del Department of Human Services. La ley prohíbe a los empleados de DHS proporcionar asesoría legal.
ENTER ADDRESSEE NAME
ENTER ADDRESSEE CARE OF
ENTER ADDRESSEE PO BOX OR STREET
ENTER ADDRESSEE CITY/STATE/ZIP
Case Number:
Date:
DHS Office:
Specialist:
Phone:
Fax:
Specialist ID:
Department of Human Services (DHS) will not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, sex, sexual orientation, gender identity or expression, political beliefs or disability. If you need help with reading, writing, hearing, etc., under the Americans with Disabilities Act, you are invited to make your needs known to a DHS office in your area.
INSTRUCTIONS: Complete all items below. Send completed form in envelope provided or, take it to your local DHS Office.
ATTENTION: Hearing Coordinator
AH Register # |
Programs in Dispute |
|
Date Completed |
|
|
|
|
Hearing Request Date |
Hearing Scheduled? |
|
Hearing Date and Time (if scheduled) |
|
YES |
NO |
|
|
|
|
|
I DO NOT WANT A HEARING. Please cancel my request for a hearing for the following reason:
(Check the appropriate box below)
I now understand that the action taken by DHS was correct.
DHS has changed its action in my case. I am now satisfied. The change is:
Other. (You must explain)
Signature |
Telephone Number |
Date Signed |
|
( |
) |
Street Address or Route Number |
City, State, and Zip Code |
|
Department of Human Services (DHS) will not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, sex, sexual orientation, gender identity or expression, political beliefs or disability. If you need help with reading, writing, hearing, etc., under the Americans with Disabilities Act, you are invited to make your needs known to a DHS office in your area.
AUTHORITY: MCLA 400.9 |
COMPLETION: Voluntary |
A. H. Approval
Yes
No Date: