
Making use of the online PDF tool by FormsPal, you can complete or edit 4691 eng right here and now. FormsPal team is focused on providing you the perfect experience with our editor by constantly adding new features and improvements. Our editor has become a lot more intuitive as the result of the latest updates! So now, working with PDF forms is a lot easier and faster than ever. It just takes a couple of basic steps:
Step 1: Firstly, access the pdf tool by pressing the "Get Form Button" in the top section of this webpage.
Step 2: The editor gives you the capability to work with the majority of PDF forms in many different ways. Transform it by adding your own text, adjust original content, and add a signature - all within the reach of a few clicks!
It's simple to fill out the document using out practical guide! Here's what you need to do:
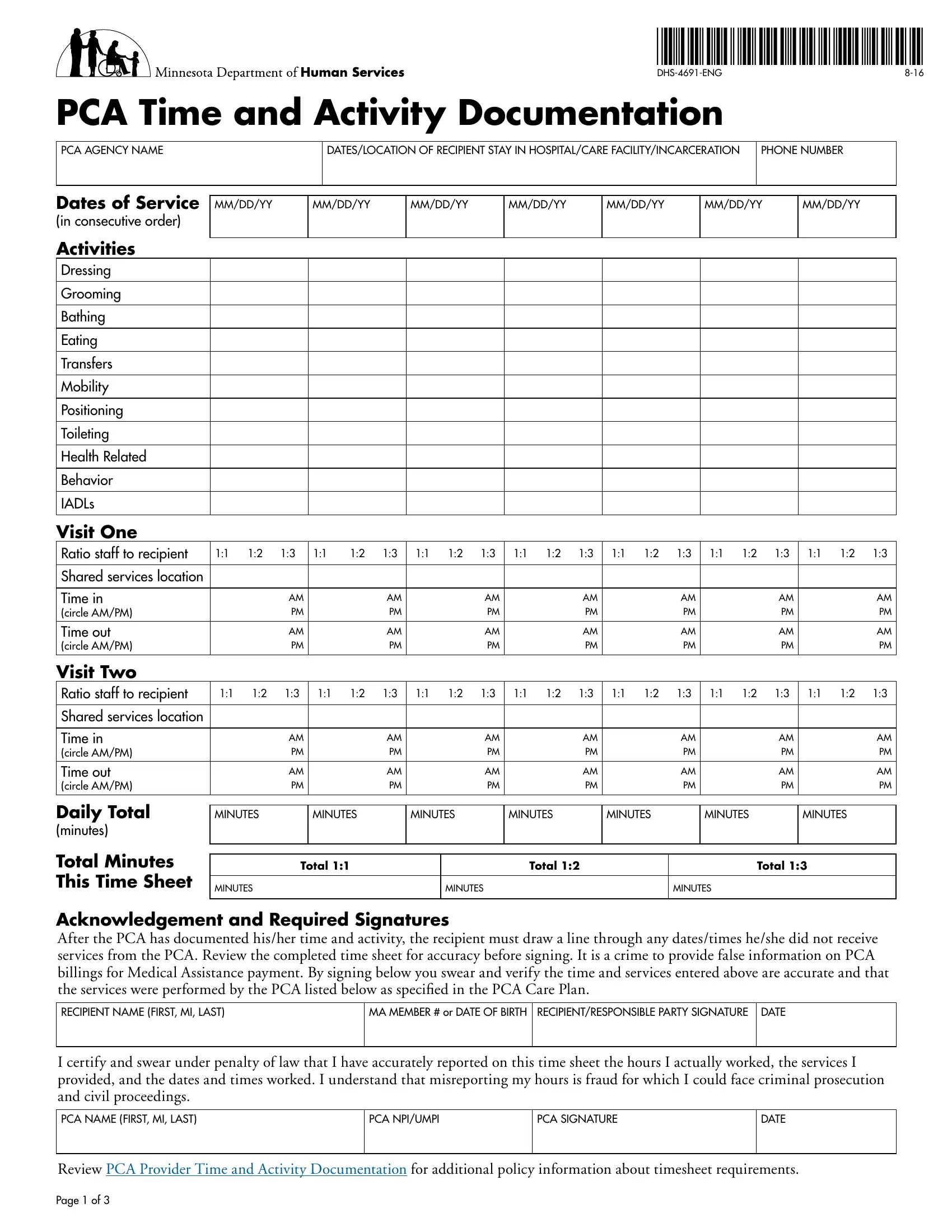
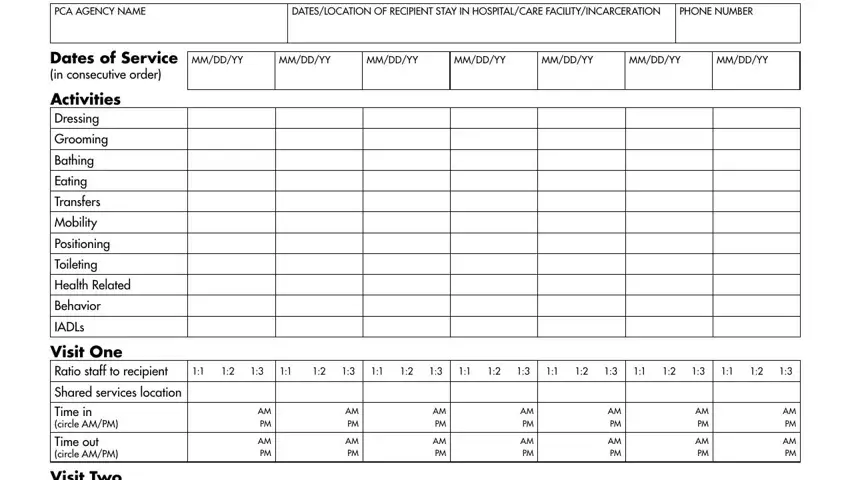
1. It is critical to complete the 4691 eng accurately, hence be attentive when working with the areas that contain all these blank fields:
2. Once this section is finished, you should insert the essential particulars in Acknowledgement and Required, MA MEMBER or DATE OF BIRTH, I certify and swear under penalty, PCA SIGNATURE, PCA NPIUMPI, DATE, Review PCA Provider Time and, and Page of so you're able to progress further.
It's very easy to get it wrong while filling out your MA MEMBER or DATE OF BIRTH, thus ensure that you take a second look prior to when you submit it.
3. Through this stage, look at PCA AGENCY PHONE NUMBER, Attention If you need free help, gkarbkEbäksarenHedaytKitfÂ, kMNtsMKal ebIGktUvkarCMnYyk, Atención Si desea recibir, and L B. Every one of these are required to be filled in with utmost accuracy.
Step 3: Immediately after looking through the entries, click "Done" and you're all set! Make a 7-day free trial plan at FormsPal and get direct access to 4691 eng - downloadable, emailable, and editable inside your FormsPal cabinet. FormsPal offers secure form editor devoid of data record-keeping or distributing. Rest assured that your details are secure with us!