
You can complete dhs 3090 form without difficulty with our PDFinity® editor. The editor is continually upgraded by our team, receiving awesome functions and growing to be even more convenient. Getting underway is effortless! Everything you need to do is adhere to the following easy steps directly below:
Step 1: Access the PDF file in our tool by pressing the "Get Form Button" in the top part of this page.
Step 2: This editor allows you to work with your PDF in a variety of ways. Transform it with any text, adjust what's originally in the document, and put in a signature - all within the reach of a couple of mouse clicks!
When it comes to fields of this precise PDF, here's what you should consider:
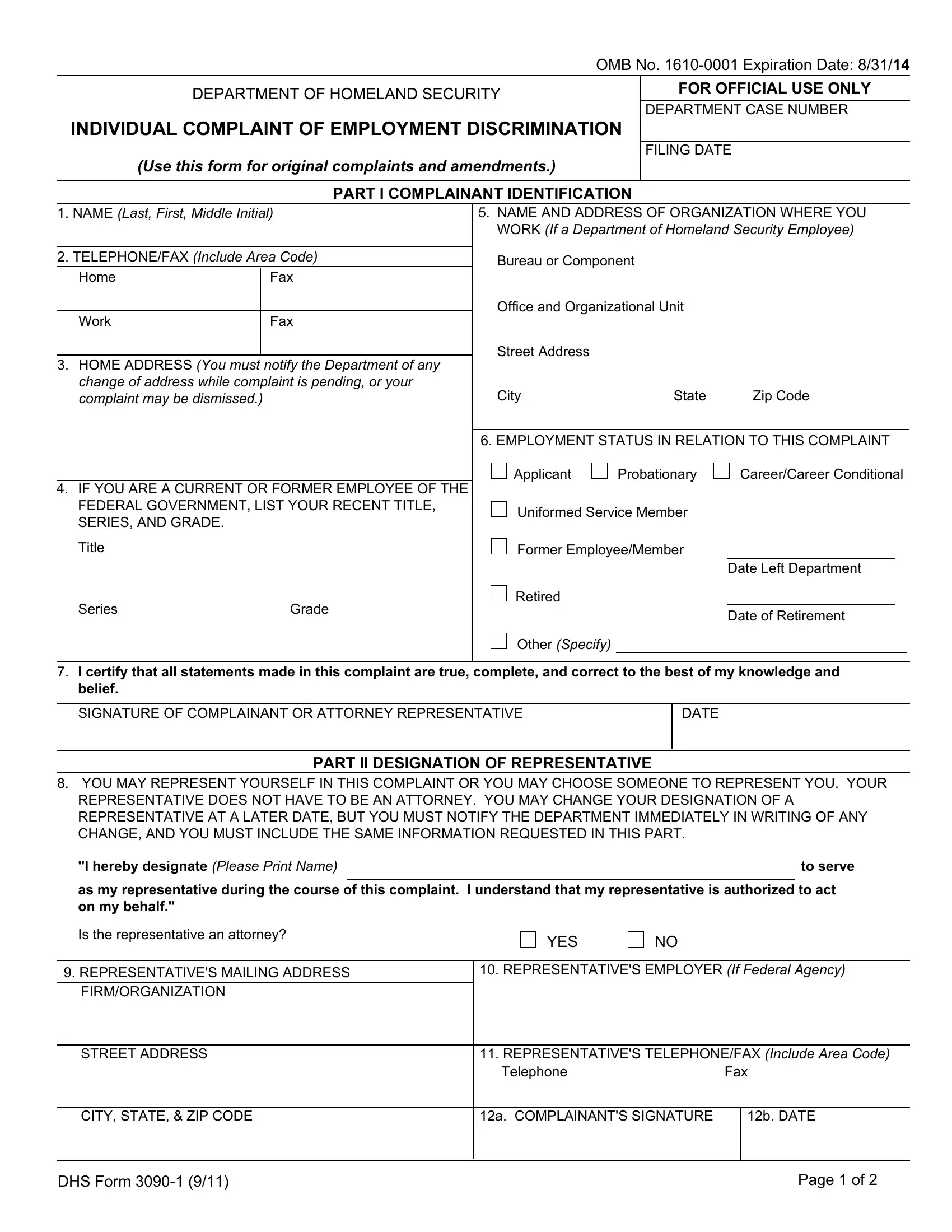
1. Before anything else, when filling in the dhs 3090 form, begin with the area that contains the following blank fields:
2. When this part is completed, go to type in the applicable information in all these: Series, Grade, Retired, Other Specify, Date Left Department, Date of Retirement, I certify that all statements made, SIGNATURE OF COMPLAINANT OR, DATE, PART II DESIGNATION OF, YOU MAY REPRESENT YOURSELF IN THIS, I hereby designate Please Print, to serve, as my representative during the, and Is the representative an attorney.
It's easy to get it wrong when filling in your Retired, for that reason you'll want to look again before you decide to send it in.
3. The following step will be about Telephone, Fax, CITY STATE ZIP CODE, a COMPLAINANTS SIGNATURE, b DATE, DHS Form, and Page of - fill out each one of these blank fields.

4. Your next subsection needs your input in the following parts: NAME OF PERSON OR DHS COMPONENT, FIRMORGANIZATION, STREET ADDRESS, CITY STATE ZIP CODE, ARE YOU WILLING TO PARTICIPATE IN, YES, A Describe the action taken, B Give the date when the action, Mark below ONLY the bases you, RACE Specify, COLOR Specify, RELIGION Specify, AGE Date of Birth, and PHYSICAL OR MENTAL DISABILITY. Ensure you provide all of the needed information to move forward.
5. As a final point, this final section is what you have to finish before using the PDF. The blank fields in this instance include the following: RELIGION Specify, NATIONAL ORIGIN Specify, SEX Specify, pregnancy, RETALIATIONREPRISAL Dates of Prior, GENETIC INFORMATION, SEXUAL ORIENTATION, PARENTAL STATUS, WHAT REMEDIAL OR CORRECTIVE, ON THIS SAME MATTER HAVE YOU, Negotiated grievance procedure, Agency grievance procedure, Merit Systems Protection Board, If you filed a grievance or appeal, and YES.
Step 3: Prior to moving on, double-check that blank fields were filled in correctly. The moment you determine that it's fine, press “Done." Join FormsPal now and easily use dhs 3090 form, prepared for download. All adjustments made by you are preserved , allowing you to change the pdf later as needed. FormsPal offers secure form editor with no personal information record-keeping or sharing. Be assured that your data is safe here!