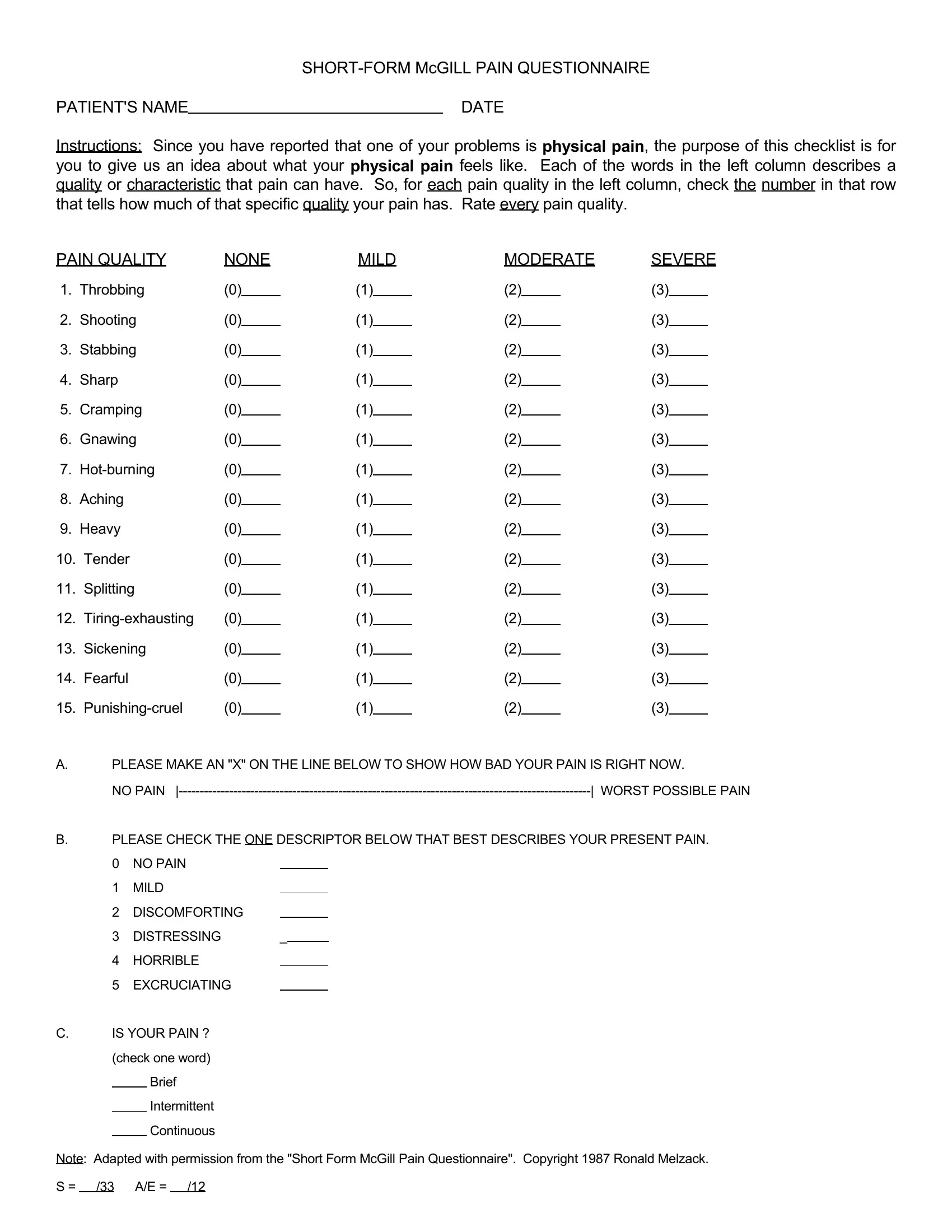
When individuals report experiencing physical pain, comprehending the intensity and nature of their discomfort becomes paramount for healthcare providers aiming to offer effective treatment. The Disability Questionnaire form, specifically the Short-Form McGill Pain Questionnaire, serves this crucial function by soliciting patients to describe their pain in detailed terms. It lists various pain qualities such as throbbing, shooting, stabbing, and cramping, among others, for the patient to evaluate in terms of intensity ranging from none to severe. Additionally, the form asks patients to mark the severity of their pain on a visual analog scale from "no pain" to "worst possible pain" and to select descriptors that best illustrate their current state of discomfort, offering options like "no pain," "mild," "discomforting," "distressing," "horrible," and "excruciating." Furthermore, it inquires about the persistence of pain, whether brief, intermittent, or continuous, providing a comprehensive view of the patient's experience. This actionable intelligence enables healthcare professionals to tailor their approaches more effectively, ensuring that the nuances of each patient's pain are adequately addressed.
| Question | Answer |
|---|---|
| Form Name | Disability Questionnaire Template Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mcgill pain questionnaire online, Copyright, checklist, mcgill pain questionnaire form printable |
PATIENT'S NAME |
|
DATE |
Instructions: Since you have reported that one of your problems is physical pain, the purpose of this checklist is for you to give us an idea about what your physical pain feels like. Each of the words in the left column describes a quality or characteristic that pain can have. So, for each pain quality in the left column, check the number in that row that tells how much of that specific quality your pain has. Rate every pain quality.
PAIN QUALITY |
NONE |
MILD |
MODERATE |
SEVERE |
|||||||||
1. |
Throbbing |
(0) |
|
|
(1) |
|
(2) |
|
|
(3) |
|
|
|
2. |
Shooting |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
||
3. |
Stabbing |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
||
4. |
Sharp |
(0) |
|
|
(1) |
|
(2) |
|
|
(3) |
|
|
|
5. |
Cramping |
(0) |
|
|
(1) |
|
(2) |
|
|
(3) |
|
|
|
6. |
Gnawing |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
||
7. |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
|||
8. |
Aching |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
||
9. |
Heavy |
(0) |
|
|
(1) |
|
(2) |
|
|
(3) |
|
|
|
10. |
Tender |
(0) |
|
|
|
(1) |
|
(2) |
|
|
(3) |
|
|
11. |
Splitting |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
||
12. |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
|||
13. |
Sickening |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
||
14. |
Fearful |
(0) |
|
|
|
(1) |
|
(2) |
|
|
(3) |
|
|
15. |
(0) |
|
(1) |
|
(2) |
|
|
(3) |
|
|
|||
A.PLEASE MAKE AN "X" ON THE LINE BELOW TO SHOW HOW BAD YOUR PAIN IS RIGHT NOW.
NO PAIN |
| WORST POSSIBLE PAIN |
B.PLEASE CHECK THE ONE DESCRIPTOR BELOW THAT BEST DESCRIBES YOUR PRESENT PAIN. 0 NO PAIN
1 MILD
2DISCOMFORTING
3 DISTRESSING |
_ |
|
4HORRIBLE
5 EXCRUCIATING
C.IS YOUR PAIN ? (check one word)
Brief Intermittent Continuous
Note: Adapted with permission from the "Short Form McGill Pain Questionnaire". Copyright 1987 Ronald Melzack. S = /33 A/E = /12