
Dealing with PDF documents online is always very simple with this PDF tool. Anyone can fill in state disability pass here within minutes. To make our editor better and easier to work with, we constantly develop new features, bearing in mind suggestions from our users. With some easy steps, you may begin your PDF editing:
Step 1: Click on the orange "Get Form" button above. It's going to open our editor so you can begin completing your form.
Step 2: With our handy PDF tool, it is possible to accomplish more than simply complete blank fields. Try all the features and make your docs look faultless with customized text put in, or fine-tune the file's original input to perfection - all comes with an ability to incorporate your personal images and sign the document off.
This PDF doc will involve some specific details; in order to guarantee correctness, remember to take note of the following guidelines:
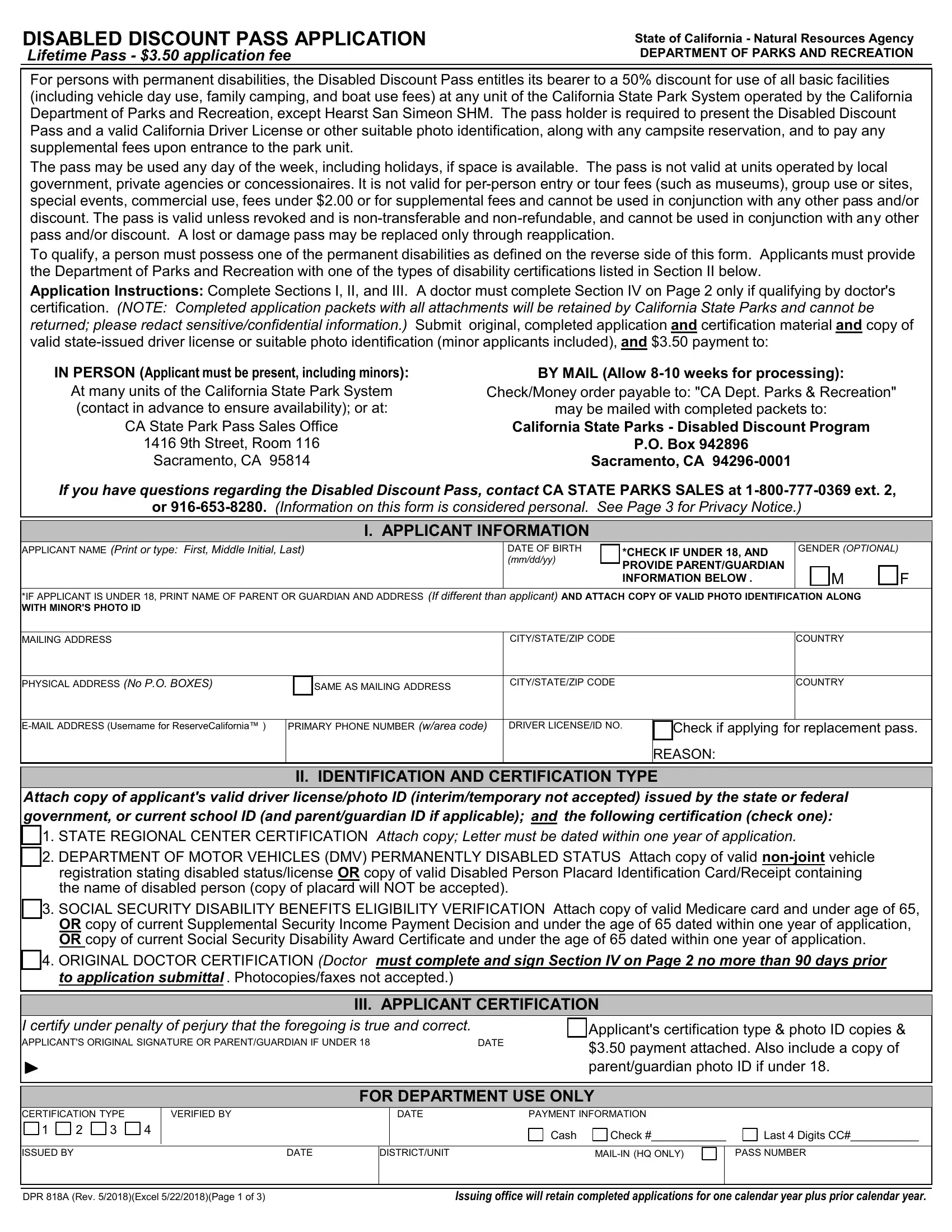
1. When submitting the state disability pass, ensure to complete all necessary blank fields within its relevant part. This will help hasten the process, enabling your information to be processed without delay and correctly.
2. Soon after filling in the last section, go to the next part and enter the necessary details in all these blanks - I certify under penalty of perjury, DATE, Applicants certification type, III APPLICANT CERTIFICATION, CERTIFICATION TYPE, VERIFIED BY, DATE, PAYMENT INFORMATION, FOR DEPARTMENT USE ONLY, Cash, Check, Last Digits CC, ISSUED BY, DATE, and DISTRICTUNIT.
3. This third section is considered pretty simple, APPLICANTPATIENT, NAME, First Middle Initial Last, DOCTORS PRINTED NAME, PROFESSIONAL LICENSE NO, BUSINESS ADDRESS, CITYSTATEZIP, BUSINESS PHONE NO Including Area, BUSINESS EMAIL ADDRESS Optional, I certify under penalty of perjury, DATE, NOTICE TO EMPLOYEES The, and DPR A Rev Excel Page of - every one of these form fields will need to be completed here.
Be really attentive when completing CITYSTATEZIP and DATE, as this is the part in which many people make some mistakes.
Step 3: Check what you have inserted in the form fields and click on the "Done" button. Get hold of the state disability pass the instant you subscribe to a free trial. Easily get access to the pdf file in your personal cabinet, with any modifications and adjustments conveniently synced! FormsPal ensures your data privacy with a secure method that never records or distributes any personal data provided. Be confident knowing your paperwork are kept safe every time you use our services!