
Dealing with PDF forms online is always a piece of cake using our PDF editor. You can fill out dmv restricted here and try out many other functions we provide. Our editor is constantly developing to provide the very best user experience attainable, and that's thanks to our commitment to continuous improvement and listening closely to comments from customers. It just takes a few easy steps:
Step 1: Access the PDF file in our editor by pressing the "Get Form Button" above on this page.
Step 2: With our advanced PDF editor, it's possible to accomplish more than just complete forms. Try all of the functions and make your docs appear faultless with custom textual content added in, or tweak the original input to excellence - all that comes along with an ability to incorporate any kind of graphics and sign the file off.
This form will need specific data to be filled out, so you need to take the time to enter what's asked:
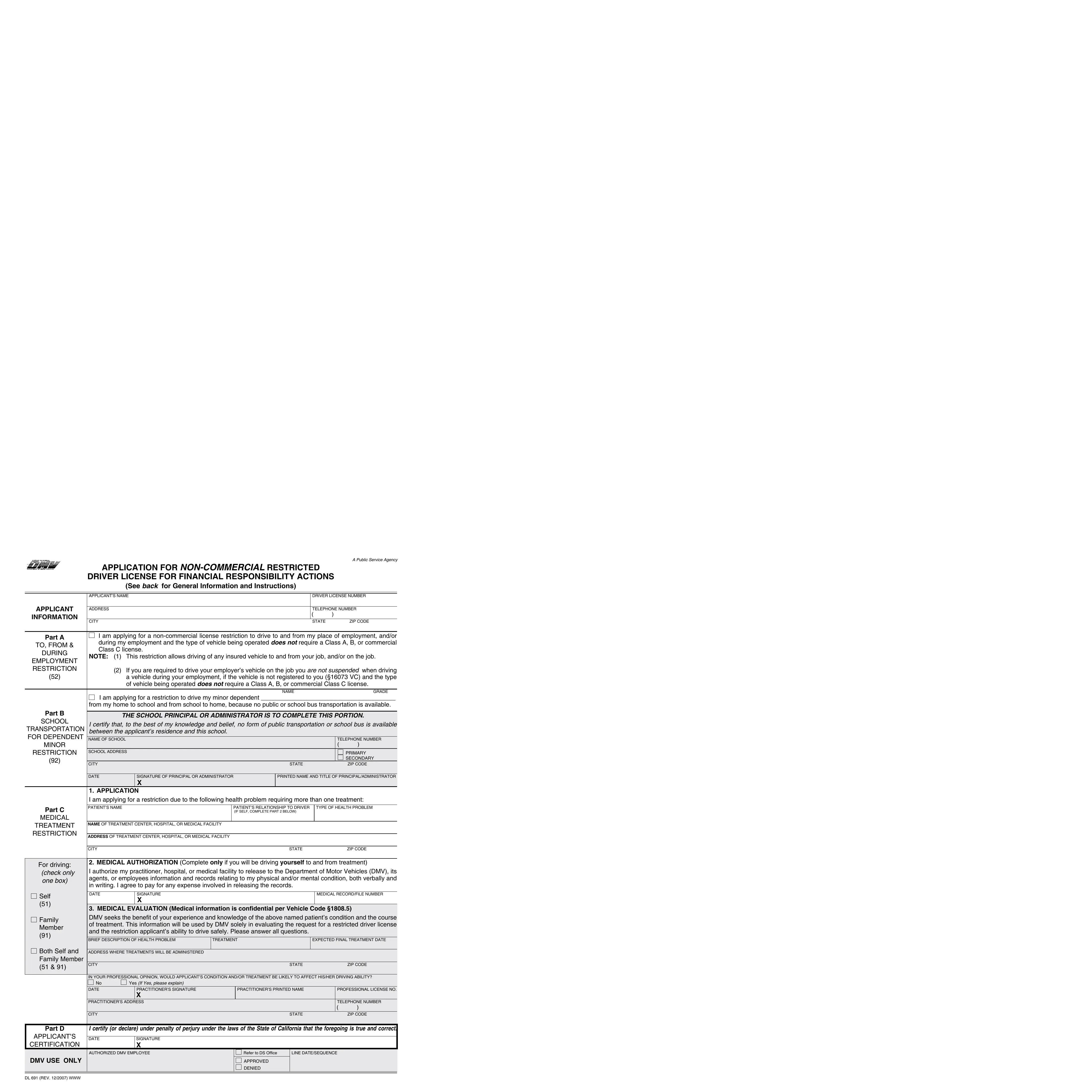
1. While completing the dmv restricted, ensure to complete all necessary blank fields in the relevant form section. It will help to facilitate the work, making it possible for your details to be processed without delay and correctly.

2. Once your current task is complete, take the next step – fill out all of these fields - SIGNATURE OF PRINCIPAL OR, TYPE OF HEALTH PROBLEM, Part C, MEDICAL, TREATMENT RESTRICTION, NAME OF TREATMENT CENTER HOSPITAL, ADDRESS OF TREATMENT CENTER, PATIENTS RELATIONSHIP TO DRIVER IF, CITY, STATE, zIP CODE, For driving check only one box, MEDICAL AUTHORIZATION Complete, Self, and Family Member with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!

3. The following section is related to Part D, I certify or declare under penalty, APPLICANTS CERTIFICATION, DATE, SIGNATURE X, DMV USE ONLY, DL REV WWW, AUTHORIzED DMV EMPLOYEE, Refer to DS Ofice, LINE DATESEqUENCE, APPROVED, and DENIED - fill out each of these blank fields.

Be really careful when filling in DL REV WWW and DMV USE ONLY, because this is where a lot of people make errors.
Step 3: Just after rereading the entries, press "Done" and you are done and dusted! Obtain your dmv restricted when you sign up for a free trial. Conveniently gain access to the form inside your FormsPal account, with any edits and changes being conveniently saved! FormsPal guarantees protected document completion with no personal data record-keeping or sharing. Rest assured that your information is secure with us!