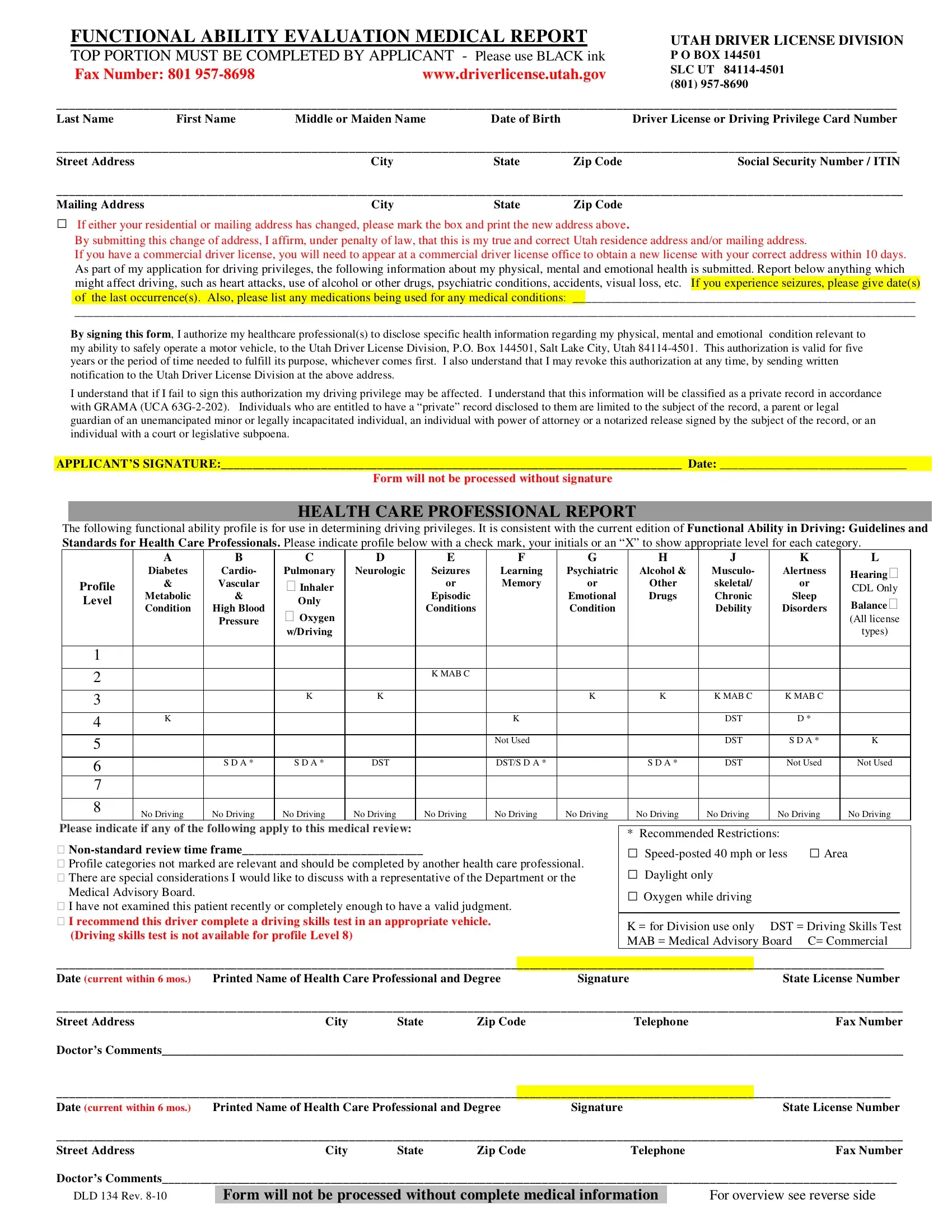
The DLD 134 form, also known as the Functional Ability Evaluation Medical Report, is an essential document for individuals seeking to apply for or renew driving privileges in Utah. It plays a pivotal role in ensuring the safety of both the applicant and the public by assessing the physical, mental, and emotional health of the driver. The form requires the applicant to provide detailed personal information, including their name, address, social security number or ITIN, and any changes to their residential or mailing address. Moreover, applicants must disclose any health conditions or medications that could affect their driving ability, such as heart conditions, use of alcohol or drugs, psychiatric conditions, visual impairments, seizures, and more. This comprehensive evaluation extends to the healthcare professional's perspective, who must fill out a functional ability profile based on current standards and guidelines, indicating any recommended restrictions or necessary tests. The DLD 134 form emphasizes the collaborative effort between the applicant, healthcare professionals, and the Utah Driver License Division to maintain road safety while addressing the individual needs of drivers.
| Question | Answer |
|---|---|
| Form Name | Dld 134 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dld 134 form, dld 134 rev 5 18, utah, DST |
FUNCTIONAL ABILITY EVALUATION MEDICAL REPORT |
UTAH DRIVER LICENSE DIVISION |
||
TOP PORTION MUST BE COMPLETED BY APPLICANT - Please use BLACK ink |
P O BOX 144501 |
||
Fax Number: 801 |
www.driverlicense.utah.gov |
SLC UT |
|
(801) |
|||
|
|
||
_______________________________________________________________________________________________________________________________________
Last NameFirst NameMiddle or Maiden NameDate of BirthDriver License or Driving Privilege Card Number
_______________________________________________________________________________________________________________________________________
Street AddressCityStateZip CodeSocial Security Number / ITIN
________________________________________________________________________________________________________________________________________
Mailing Address |
City |
State |
Zip Code |
□If either your residential or mailing address has changed, please mark the box and print the new address above.
By submitting this change of address, I affirm, under penalty of law, that this is my true and correct Utah residence address and/or mailing address.
If you have a commercial driver license, you will need to appear at a commercial driver license office to obtain a new license with your correct address within 10 days. As part of my application for driving privileges, the following information about my physical, mental and emotional health is submitted. Report below anything which might affect driving, such as heart attacks, use of alcohol or other drugs, psychiatric conditions, accidents, visual loss, etc. If you experience seizures, please give date(s) of the last occurrence(s). Also, please list any medications being used for any medical conditions: _______________________________________________________
_______________________________________________________________________________________________________________________________________
By signing this form, I authorize my healthcare professional(s) to disclose specific health information regarding my physical, mental and emotional condition relevant to my ability to safely operate a motor vehicle, to the Utah Driver License Division, P.O. Box 144501, Salt Lake City, Utah
I understand that if I fail to sign this authorization my driving privilege may be affected. I understand that this information will be classified as a private record in accordance with GRAMA (UCA
APPLICANT’S SIGNATURE:__________________________________________________________________________ Date: ______________________________
Form will not be processed without signature
HEALTH CARE PROFESSIONAL REPORT
The following functional ability profile is for use in determining driving privileges. It is consistent with the current edition of Functional Ability in Driving: Guidelines and Standards for Health Care Professionals. Please indicate profile below with a check mark, your initials or an “X” to show appropriate level for each category.
Profile Level
1
2
3
4
5
6
7
8
A
Diabetes
&
Metabolic
Condition
K
No Driving
B
Cardio-
Vascular
&
High Blood
Pressure
S D A *
No Driving
C
Pulmonary
Inhaler Only
Oxygen w/Driving
K
S D A *
No Driving
D
Neurologic
K
DST
No Driving
E
Seizures
or
Episodic
Conditions
K MAB C
No Driving
F
Learning Memory
K
Not Used
DST/S D A *
No Driving
G
Psychiatric
or
Emotional
Condition
K
No Driving
H
Alcohol &
Other
Drugs
K
S D A *
No Driving
J
Musculo-
skeletal/
Chronic
Debility
K MAB C
DST
DST
DST
No Driving
K
Alertness
or
Sleep
Disorders
K MAB C
D*
S D A *
Not Used
No Driving
L
Hearing
CDL Only
Balance
(All license
types)
K
Not Used
No Driving
Please indicate if any of the following apply to this medical review:
Profile categories not marked are relevant and should be completed by another health care professional.
There are special considerations I would like to discuss with a representative of the Department or the Medical Advisory Board.
I have not examined this patient recently or completely enough to have a valid judgment.
I recommend this driver complete a driving skills test in an appropriate vehicle. (Driving skills test is not available for profile Level 8)
* Recommended Restrictions:
□
□Daylight only
□Oxygen while driving
K = for Division use only DST = Driving Skills Test MAB = Medical Advisory Board C= Commercial
_____________________________________________________________________________________________________________________________________
Date (current within 6 mos.) Printed Name of Health Care Professional and DegreeSignatureState License Number
________________________________________________________________________________________________________________________________________
Street AddressCityStateZip CodeTelephoneFax Number
Doctor’s Comments________________________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________________
Date (current within 6 mos.) Printed Name of Health Care Professional and DegreeSignatureState License Number
________________________________________________________________________________________________________________________________________
Street Address |
City |
State |
Zip Code |
Telephone |
Fax Number |
|
Doctor’s Comments______________________________________________________________________________________________________________________ |
||||||
DLD 134 Rev. |
Form will not be processed without complete medical information |
|
For overview see reverse side |
|||

FOR USE AS AN OVERVIEW ONLY
Functional ability profiles serve to define a person’s physical, mental, or emotional health in a way that it can easily be related to issuing regular or restricted driver licenses.
This table shows, in general, the principle requirements for each level and may be used as a rough guide only. A full narrative description and table for each category are found in the
Functional Ability In Driving: Guidelines and Standards for Health Care Professionals, which is available at a Utah Driver License Division office or
Level |
|
A |
|
B |
|
C |
|
D |
|
E |
|
F |
|
G |
|
H |
|
|
I |
|
|
Diabetes & |
|
Cardio- |
|
Pulmonary |
|
Neurologic |
|
Seizures & |
|
Learning |
|
Psychiatric |
|
Alcohol & |
|
Visual |
|
|
|
Metabolic |
|
vascular |
|
|
|
|
|
Episodic |
|
Memory |
|
Emotional |
|
Other Drugs |
|
Acuity |
|
|
|
Conditions |
|
|
|
|
|
|
|
Conditions |
|
|
|
Condition |
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No history |
|
No past history |
|
No disease |
|
No history or |
|
No history or |
|
No history or |
|
No history or |
|
No history or |
|
|
|
|
|
|
|
|
or fully |
|
or fully |
|
fully |
|
none in 5 |
|
fully |
|
no symptoms |
|
no problems |
|
|
|
|
|
|
|
recovered |
|
recovered |
|
recovered |
|
years w/o |
|
recovered |
|
for 2 years |
|
within 2 years |
|
AONCOMPLETEDBE |
EXAMINATION"VISUAL |
|
|
|
|
|
|
|
|
|
|
medication |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
Adult, stable |
|
All Class I |
|
Minimal |
|
Minimal |
|
Seizure free 1 |
|
Minimal |
|
Stable 1 year |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
with non- |
|
rhythm, no |
|
symptoms. |
|
impairment, |
|
year, off |
|
difficulty |
|
with or |
|
consequences |
|
|
|
|
|
insulin |
|
limits, no |
|
No steroids |
|
able to |
|
medication |
|
with good |
|
without |
|
within past |
|
|
|
|
|
stimulation, |
|
symptoms on |
|
|
|
control |
|
|
|
adjustment |
|
medication |
|
year |
|
|
|
|
|
diet and/or |
|
ordinary |
|
|
|
equipment |
|
|
|
|
|
|
|
|
|
|
|
|
|
oral meds |
|
activity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
Stable on oral |
|
Class I rhythm |
|
Symptoms |
|
Slight |
|
Seizure free 1 |
|
Slight |
|
Stable 3 |
|
No |
|
|
|
|
|
insulin- |
|
stable, with |
|
on activity, |
|
impairment, |
|
year, on |
|
impairment |
|
months with |
|
consequences |
|
|
|
|
|
stimulating |
|
pacemaker for |
|
intermittent |
|
able to |
|
medication |
|
with good |
|
or without |
|
within past 6 |
|
|
|
|
|
agent and/or |
|
6 months |
|
steroids FVC |
|
control |
|
|
|
judgment |
|
medication |
|
months |
|
|
|
|
|
diet |
|
Symptoms with |
|
& FEV>50% |
|
equipment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
strenuous |
|
of normal |
|
|
|
|
|
|
|
|
|
|
|
SHOULDPROFILE |
"CERTIFICATEOF |
|
|
|
|
activity |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
4 |
|
Stable on |
|
Class II rhythm, |
|
Stable with |
|
Moderate |
|
Seizure free 6 |
|
Moderate |
|
Stable 1 |
|
No |
|
||
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
insulin for 1 |
|
stable for 3 |
|
O2 or |
|
impairment |
|
months on |
|
impairment |
|
month with |
|
consequences |
|
|
|
|
|
year |
|
months |
|
steroids, |
|
of dexterity |
|
medication |
|
with good |
|
medication |
|
within past 3 |
|
|
|
|
|
|
|
Diastolic under |
|
dyspnea on |
|
|
|
|
|
judgment |
|
|
|
months |
|
|
|
|
|
|
120 |
|
exertion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
Stable for 6 |
|
Class III |
|
PO2 over 50, |
|
Moderate |
|
Seizure free 3 |
|
|
|
Minimal |
|
No |
|
|
|
|
|
months |
|
anticipated |
|
symptoms |
|
impairment |
|
months on |
|
|
|
dyskinesia, |
|
consequences |
|
|
|
|
|
|
|
aggravation by |
|
w/ordinary |
|
and |
|
medication |
|
|
|
medications |
|
within past 1 |
|
CATEGORYTHIS |
FORM:SEPARATE |
|
|
|
|
unlimited |
|
activity, no |
|
decreased |
|
|
|
NOT USED |
|
which |
|
month |
|
||
|
|
|
|
driving |
|
cough |
|
stamina |
|
|
|
|
|
interfere with |
|
|
|
|
|
|
|
|
|
|
|
syncope 3 |
|
|
|
|
|
|
|
coordination |
|
|
|
|
|
|
|
|
|
|
|
months |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
Stable for 3 |
|
Class III |
|
Severe |
|
Moderate |
|
Single |
|
Moderate |
|
As |
|
Intermittent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
months |
|
unstable |
|
dyspnea no |
|
impairment |
|
recurrence |
|
impairment, |
|
recommended. |
|
impairment of |
|
|
|
|
|
|
|
rhythm, |
|
syncope |
|
expected to |
|
over 2 years |
|
variable |
|
Driving under |
|
function, not |
|
|
|
|
|
|
|
uncontrolled |
|
within 3 |
|
be temporary |
|
Special |
|
adjustment |
|
direct |
|
in driving or |
|
|
|
|
|
|
|
hypertension |
|
months |
|
|
|
circumstances |
|
or altered |
|
supervision |
|
working |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
competence |
|
may be |
|
hours, drive |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
from meds, |
|
therapeutic |
|
under |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
alcohol,drugs |
|
|
|
supervision |
|
|
|
7 |
|
|
|
|
|
|
|
|
|
Special Circumstances or under evaluation |
|
|
|
||||||
8 |
|
Severe |
|
Class IV |
|
Severe |
|
Impairment |
|
Seizures not |
|
Severe |
|
Active |
|
Chronic use |
|
Level 10 |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
unstable |
|
arrhythmia with |
|
dyspnea, |
|
incompatible |
|
controlled or |
|
impairment |
|
condition with |
|
of alcohol or |
|
20/200 or |
|
|
|
insulin- |
|
loss of |
|
syncope |
|
w/driving |
|
interfering |
|
and poor |
|
risk |
|
drugs |
|
worse |
|
|
|
dependant |
|
conscious |
|
within 3 |
|
|
|
medications, |
|
adjustment |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
with VF |
||||||
|
|
|
|
uncontrolled |
|
months |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
less than |
|||
|
|
|
|
Ht, |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
60 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
NOb |
|
NO |
|
NO |
|
NO |
|
NO |
|
NO |
|
NO |
|
NO |
|
degrees |
|
|
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
NO DRIV |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
J |
|
K |
|
L |
|
Musculo- |
|
Alertness & |
|
Hearinga |
|
skeletal or |
|
Sleep |
|
(CDL only) & |
|
Chronic |
|
Disorders |
|
Balance |
|
Debility |
|
|
|
(All lic types) |
|
No history or |
|
No history or |
|
No current or |
|
fully recovered |
|
problem for 2 |
|
past balance |
|
1 year or more |
|
years. ESS <6 |
|
problem |
|
|
|
|
|
|
|
Minimal loss |
|
Problems with |
|
Mild balance |
|
of function |
|
good self- |
|
(Meniere’s |
|
|
|
management |
|
disease) |
|
|
|
ESS |
|
|
|
|
|
|
|
|
|
Mild loss of |
|
Mild/moderate |
|
Problems but |
|
function with |
|
problems, |
|
not |
|
or without |
|
good |
|
incapacitating |
|
compensatory |
|
professional |
|
|
|
device |
|
management |
|
|
|
|
|
ESS |
|
|
|
|
|
|
|
|
|
Moderate loss |
|
Moderate |
|
Recurring |
|
of function |
|
problems |
|
problem, not in |
|
with or |
|
related to time |
|
past 3 months |
|
without comp |
|
of day |
|
|
|
device |
|
ESS |
|
|
|
|
|
|
|
|
|
Limited joint |
|
Moderate |
|
Recurring |
|
motion |
|
problems |
|
problems not in |
|
|
|
related to time |
|
past 1 month |
|
|
|
and |
|
|
|
|
|
circumstances |
|
|
|
|
|
ESS |
|
|
|
|
|
|
|
|
|
Impairment or |
|
|
|
|
|
debility |
|
|
|
|
|
requiring |
|
|
|
|
|
assistance of |
|
NOT USED |
|
NOT USED |
|
responsible |
|
|
|
|
|
driver |
|
|
|
|
|
Chronic unsafe |
|
Severe |
|
Chronic |
|
|
|
|||
|
|
|
|||
|
conditions |
|
problem, no |
|
balance |
|
|
|
medication or |
|
problems |
|
|
|
unsuccessful |
|
|
|
|
|
therapy |
|
|
|
NO |
|
NO |
|
NO |
|
DRIVING |
|
DRIVING |
|
DRIVING |
|
|
|
|
|
|
bDriving skills test is not allowed for a profile level 8 |
a Hearing should only be profiled for a commercial driver – No hearing requirements have been established for Regular Operator Licenses |
Revised