

If you wish to fill out Dld6A Form, you don't need to download and install any sort of programs - simply use our online PDF editor. In order to make our editor better and easier to use, we constantly develop new features, taking into consideration feedback from our users. In case you are seeking to begin, here's what it's going to take:
Step 1: Just click on the "Get Form Button" above on this site to open our pdf file editor. There you will find all that is needed to fill out your file.
Step 2: This editor offers the capability to customize your PDF form in a variety of ways. Improve it by writing personalized text, correct what is already in the document, and include a signature - all close at hand!
It's straightforward to finish the pdf using out detailed tutorial! Here's what you have to do:
1. Complete the Dld6A Form with a selection of necessary blank fields. Consider all the required information and ensure absolutely nothing is neglected!
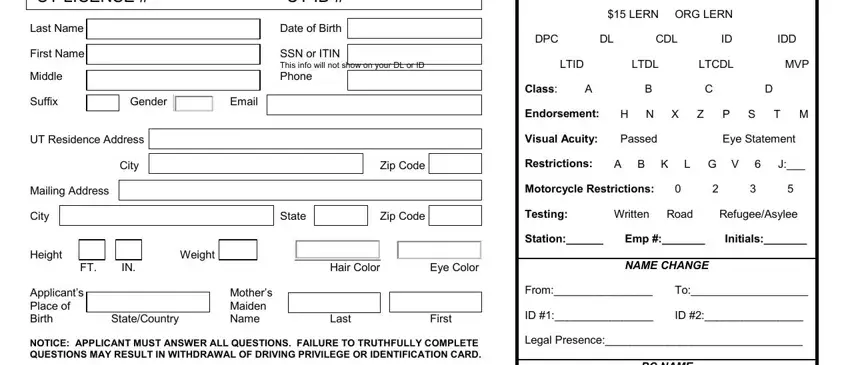
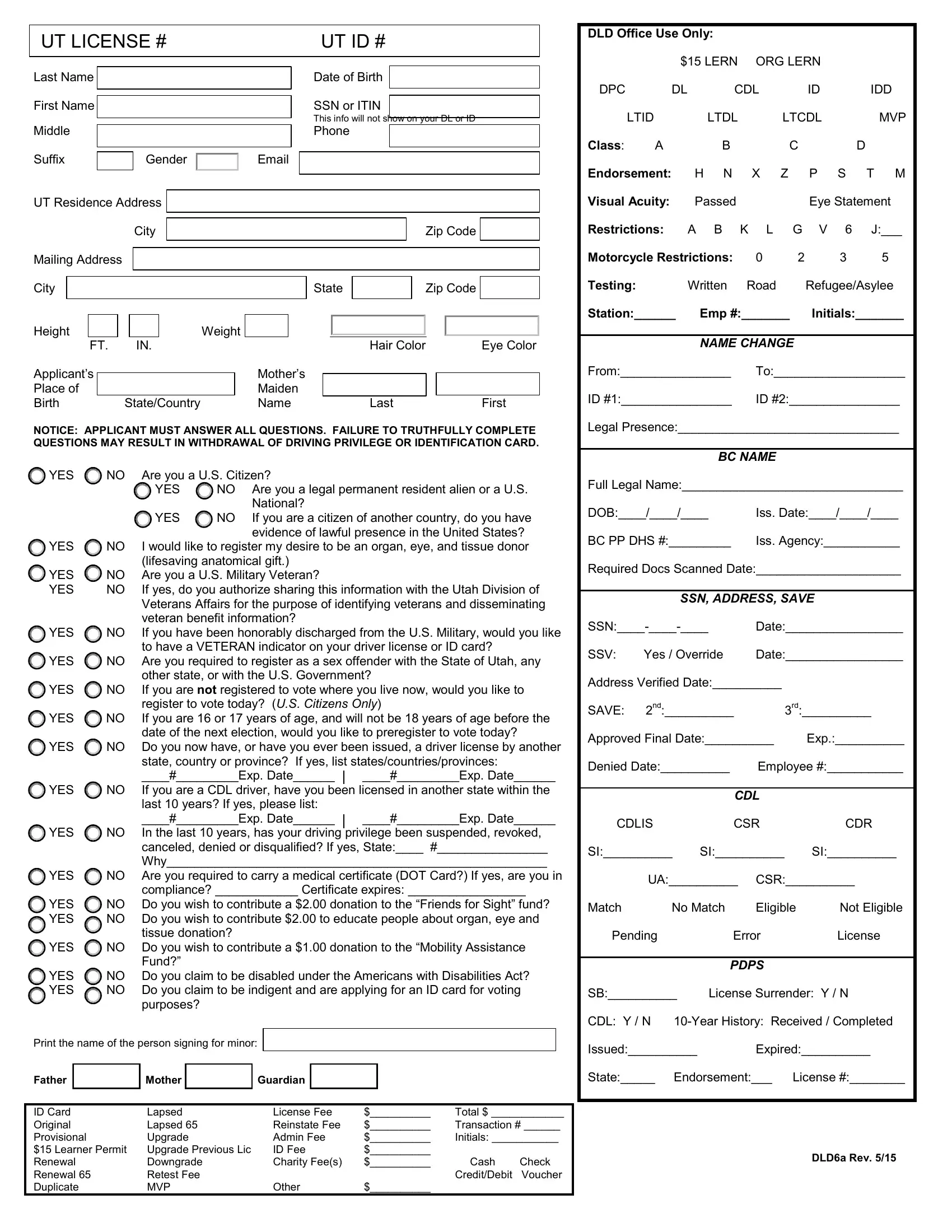
2. After the last segment is finished, you're ready to insert the necessary particulars in Last Name First Name Middle Suffix, YES, NO Are you a US Citizen, YES, NO Are you a legal permanent, YES, YES, National If you are a citizen of, YES YES, NO Are you a US Military Veteran NO, YES, NO Are you required to register as, If yes do you authorize sharing, other state or with the US, and YES so you can move forward to the third part.
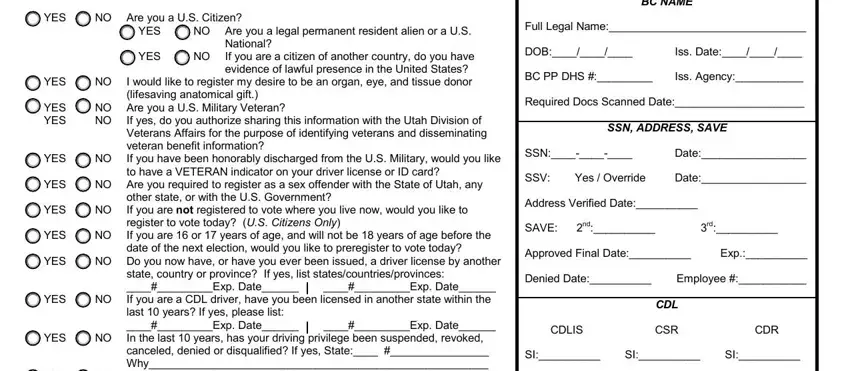
As for NO Are you a US Citizen and YES, be sure you review things in this current part. These two are the key fields in the form.
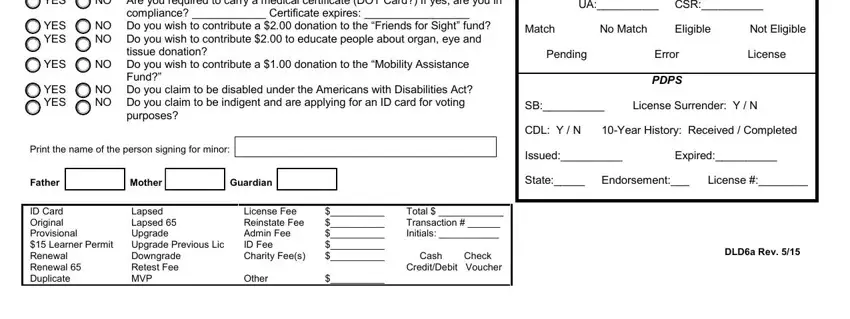
3. The next section is normally quite simple, YES, NO Are you required to carry a, YES YES, YES, compliance Certificate expires, NO Do you wish to contribute a, tissue donation, NO Do you wish to contribute a, Fund, YES YES, NO Do you claim to be disabled, purposes, UA CSR, Match, and No Match - all of these form fields will have to be filled in here.
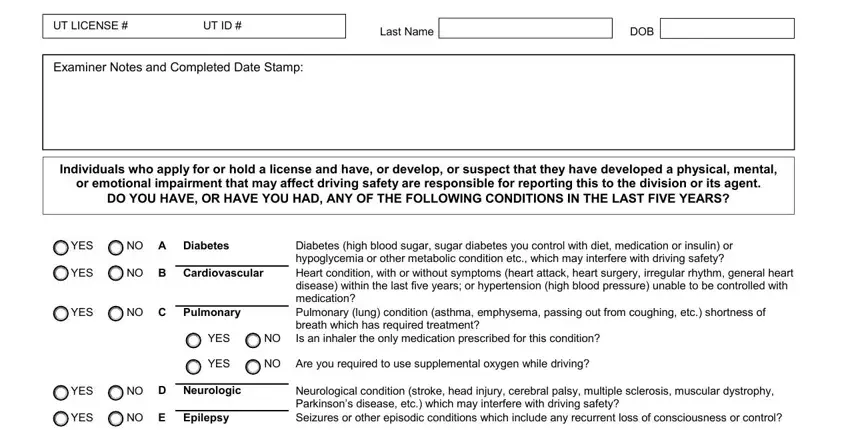
4. This next section requires some additional information. Ensure you complete all the necessary fields - UT LICENSE, UT ID, Last Name, DOB, Examiner Notes and Completed Date, Individuals who apply for or hold, or emotional impairment that may, DO YOU HAVE OR HAVE YOU HAD ANY OF, YES, NO A Diabetes, YES, NO B Cardiovascular, YES, NO C Pulmonary, and YES - to proceed further in your process!
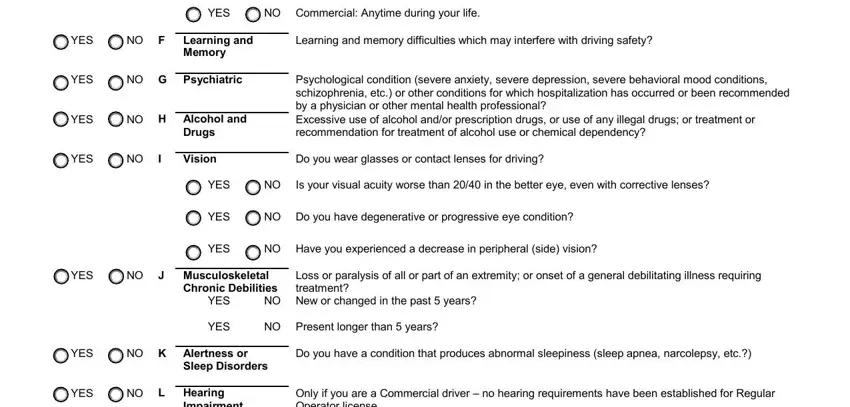
5. Lastly, the following last subsection is what you have to wrap up prior to closing the form. The fields in question include the following: YES, NO Commercial Anytime during your, Learning and memory difficulties, Psychological condition severe, Do you wear glasses or contact, Do you have degenerative or, YES, NO F, Learning and Memory, YES, NO G Psychiatric, YES, NO H Alcohol and, YES, and Drugs Vision.
Step 3: After taking another look at your entries, hit "Done" and you're all set! Make a free trial option with us and get instant access to Dld6A Form - downloadable, emailable, and editable in your personal cabinet. FormsPal is committed to the privacy of all our users; we make sure that all personal information going through our tool is kept confidential.