
pcs physician authorization for certification and treatment can be filled out easily. Simply open FormsPal PDF editing tool to get the job done without delay. Our team is dedicated to providing you the perfect experience with our tool by constantly presenting new functions and enhancements. With these improvements, working with our tool becomes better than ever before! Starting is easy! Everything you need to do is take the following easy steps directly below:
Step 1: Just click on the "Get Form Button" above on this webpage to start up our pdf form editing tool. There you will find all that is necessary to fill out your file.
Step 2: With this advanced PDF tool, you can actually accomplish more than merely fill in blank form fields. Express yourself and make your docs seem faultless with custom textual content added in, or tweak the original input to perfection - all that comes with the capability to incorporate just about any images and sign it off.
When it comes to blanks of this particular document, here's what you need to know:
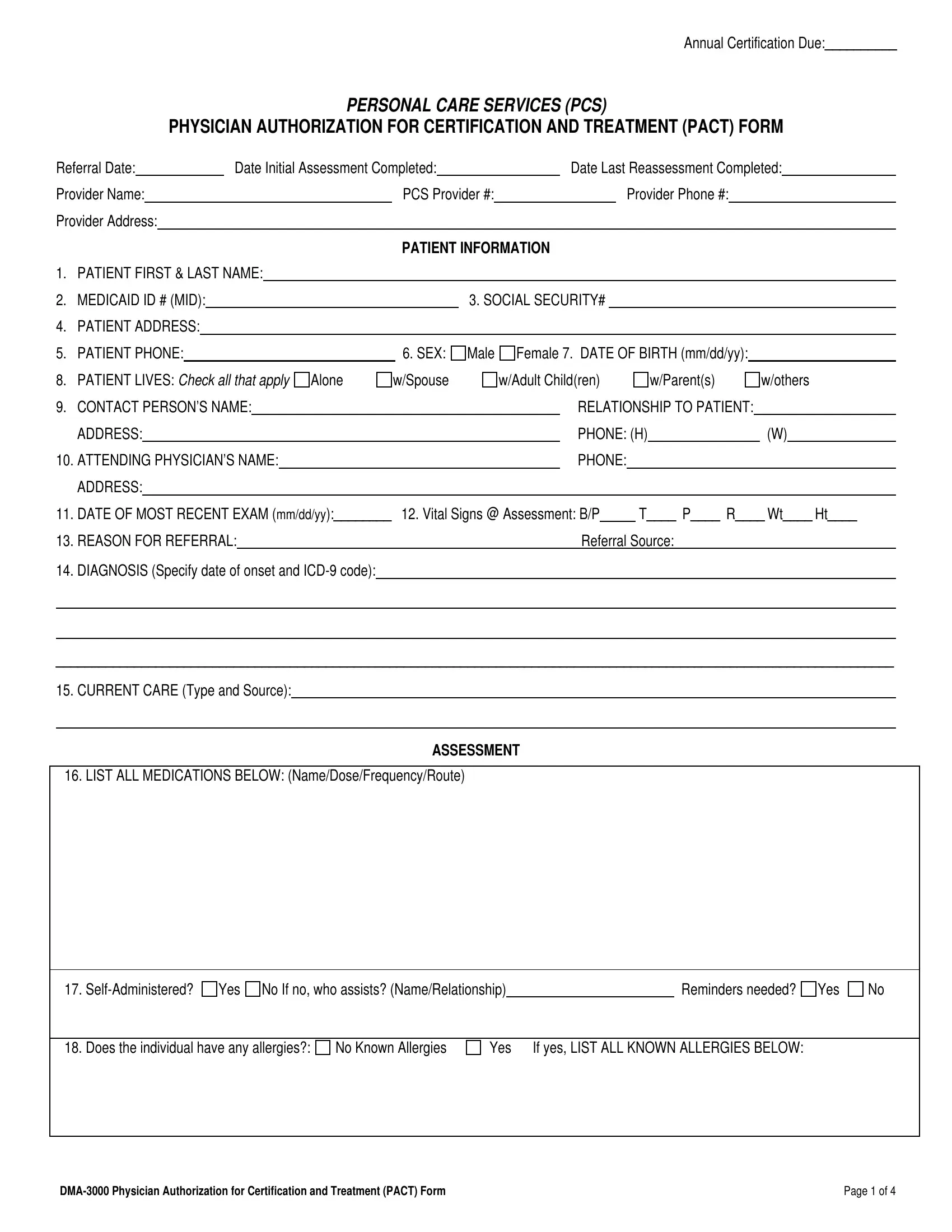
1. It's important to fill out the pcs physician authorization for certification and treatment accurately, therefore be careful when filling in the parts containing these specific blank fields:
2. The next stage is usually to fill out these blank fields: ADDRESS, DATE OF MOST RECENT EXAM mmddyy, REASON FOR REFERRAL, DIAGNOSIS Specify date of onset, Referral Source, CURRENT CARE Type and Source, ASSESSMENT, LIST ALL MEDICATIONS BELOW, SelfAdministered, Yes No If no who assists, Reminders needed, and Yes.
3. The next part is straightforward - fill in all the empty fields in No Known Allergies, Yes If yes LIST ALL KNOWN, Does the individual have any, DMA Physician Authorization for, and Page of to complete this process.
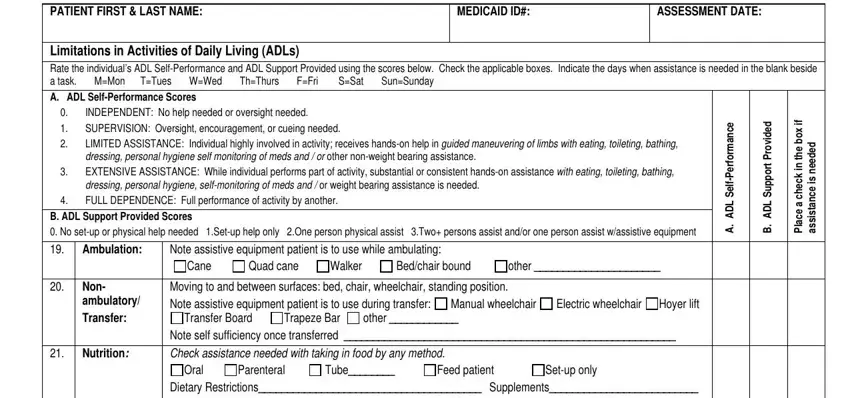
4. This next section requires some additional information. Ensure you complete all the necessary fields - PATIENT FIRST LAST NAME, MEDICAID ID, ASSESSMENT DATE, Limitations in Activities of Daily, A ADL SelfPerformance Scores, INDEPENDENT No help needed or, B ADL Support Provided Scores No, Ambulation, Note assistive equipment patient, Quad cane Walker, Bedchair bound, other, Non ambulatory Transfer, Moving to and between surfaces bed, and Manual wheelchair - to proceed further in your process!
5. The last notch to submit this document is essential. Ensure you fill out the appropriate form fields, such as Respiration, Endurance, Dietary Restrictions Supplements, Normal Dyspneic with minimal, meal, Oxygen Continuous A Dust B Vacuum, Intermittent Nebulizer Treatments, Pt is never short of breath SOB, Pt is SOB when walking more than, Pt is SOB at rest, A Change bed linens B Make bed C, Skin, Normal Dry cracked or bleeding, Pressure areas Decubiti, and Bathing, before submitting. Neglecting to do it may lead to an unfinished and probably incorrect paper!
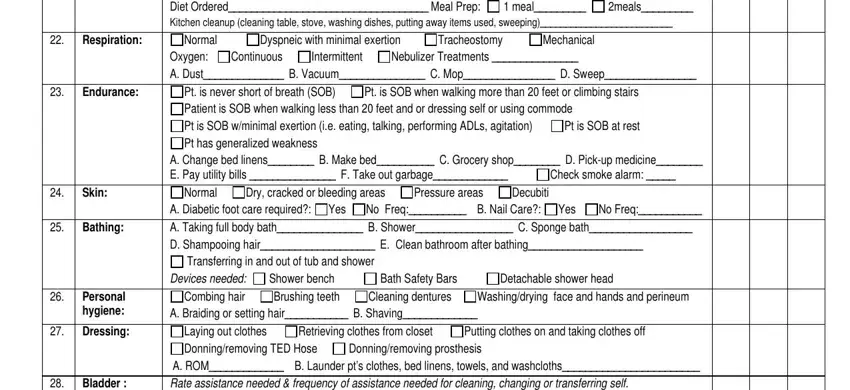
Be really mindful when filling out Oxygen Continuous A Dust B Vacuum and Endurance, because this is the part where many people make a few mistakes.
Step 3: Before moving forward, ensure that all form fields are filled out right. The moment you verify that it is good, click on “Done." Right after registering afree trial account at FormsPal, you will be able to download pcs physician authorization for certification and treatment or email it at once. The file will also be at your disposal through your personal account page with all of your modifications. We do not share any information that you type in while completing forms at our site.