The DMA-6 form helps Georgia Medicaid understand a person’s medical needs and how those needs affect daily life. A doctor fills out the form after examining the individual. Medicaid then uses the doctor’s assessment to decide whether the person needs care at an institutional level.
The form explains how medical conditions impact everyday activities. It shows whether someone has trouble moving around, taking care of themselves, or staying safe without regular help. Reviewers look at this information to decide if care in a nursing facility or an ICF/IID is needed, or if the person could be supported in another setting.
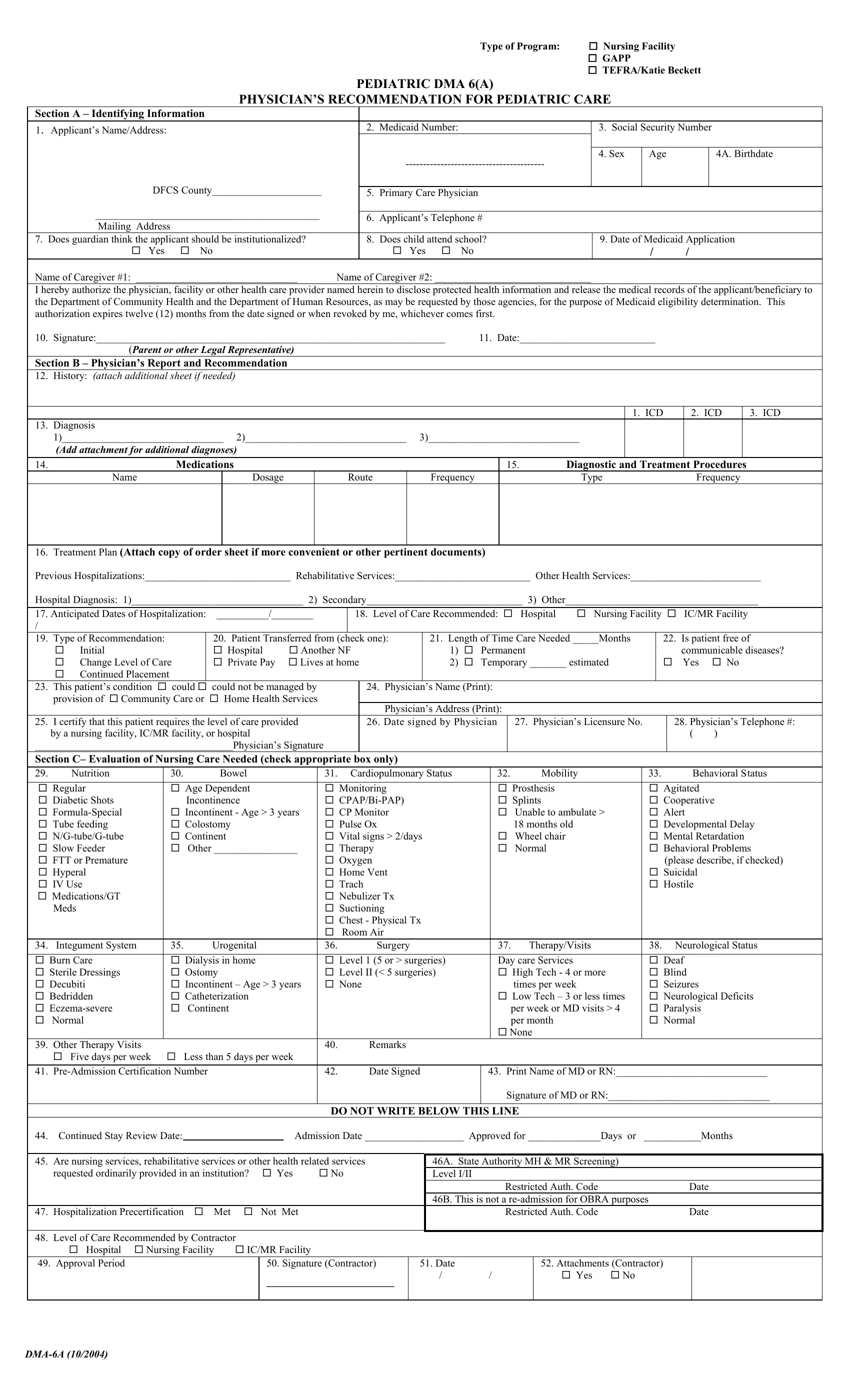
The DMA-6 includes details about the person’s health and care needs, such as:
• Current and past medical conditions
• Medications and ongoing treatments
• Hospitalizations or major medical events
• Physical, cognitive, and functional challenges
• How much nursing care or hands-on help is needed
The doctor also notes whether the care is needed for a short time or long term and recommends the right level of care. This helps Medicaid understand how much support the person is expected to need and for how long.
The doctor’s signature confirms that the information is based on an actual medical exam.
In short, any adult whose Medicaid eligibility depends on showing a medical need for long-term or institutional-level care will need a DMA-6 form.
Important note: The DMA-6 form is used for adults. For children, Medicaid uses the DMA-6A form, which is designed to evaluate pediatric medical needs and required levels of care.
| Question | Answer |
|---|---|
| Form Name | DMA 6 Form Georgia |
| Form Length | 1 page |
| Fillable? | Yes |
| Fillable fields | 100 |
| Avg. time to fill out | 15 min |
| Other names | dma6, Georgia dma-6 form for nursing home, dma-6 form Georgia, GAMMIS dma 6 form |