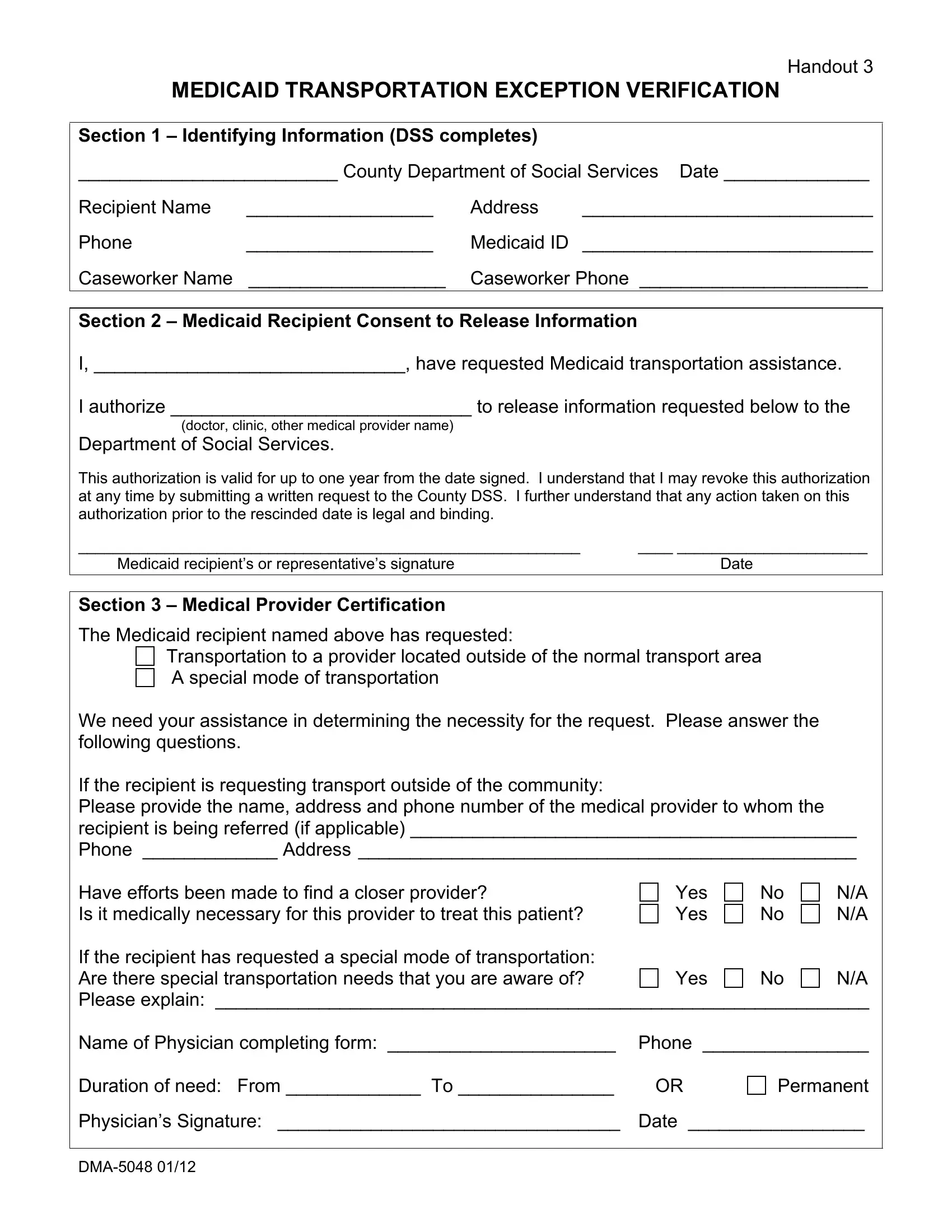
The DMA-5048 form serves as a critical document within the framework of Medicaid, facilitating a process that might otherwise seem daunting for recipients in need of transportation services for medical purposes. This form bridges the gap between Medicaid recipients, their healthcare providers, and the Department of Social Services, ensuring that those who require transportation assistance for healthcare services are properly vetted and authorized. Central to this process is the collection of identifiable information from the recipient, including their name, address, and Medicaid ID, which the Department of Social Services uses to manage requests efficiently. Furthermore, the form encapsulates a consent section where the recipient authorizes the release of necessary information to the Department of Social Services, underscoring the importance of privacy and the recipient's autonomy in disclosing personal medical information. Moreover, it introduces a medical provider certification section, which is pivotal for evaluating the necessity and specifics of the transportation request, including whether the transportation is for accessing services outside the recipient's normal transport area or requires a special mode of transportation due to specific medical needs. This segment of the form also delves into whether attempts were made to find a closer provider and the medical necessity for the specific provider requested, hence ensuring that the provision of transportation services is both necessary and efficient. Finally, the form must be signed and dated by both the Medicaid recipient or their representative and the physician, underscoring the collaborative effort between patients, healthcare providers, and social services to facilitate essential medical transportation.
| Question | Answer |
|---|---|
| Form Name | Dma 5048 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form dma 5048, dma 5048 form, dma form 5048, dma5048 form |
Handout 3
MEDICAID TRANSPORTATION EXCEPTION VERIFICATION
Section 1 – Identifying Information (DSS completes)
_________________________ County Department of Social Services Date ______________
Recipient Name |
__________________ |
Address |
____________________________ |
Phone |
__________________ |
Medicaid ID |
____________________________ |
Caseworker Name |
___________________ |
Caseworker Phone ______________________ |
|
Section 2 – Medicaid Recipient Consent to Release Information
I, ______________________________, have requested Medicaid transportation assistance.
I authorize _____________________________ to release information requested below to the
Department of Social Services.
This authorization is valid for up to one year from the date signed. I understand that I may revoke this authorization at any time by submitting a written request to the County DSS. I further understand that any action taken on this authorization prior to the rescinded date is legal and binding.
__________________________________________________________ |
____ ______________________ |
Medicaid recipient’s or representative’s signature |
Date |
Section 3 – Medical Provider Certification
The Medicaid recipient named above has requested:
Transportation to a provider located outside of the normal transport area A special mode of transportation
We need your assistance in determining the necessity for the request. Please answer the following questions.
If the recipient is requesting transport outside of the community:
Please provide the name, address and phone number of the medical provider to whom the recipient is being referred (if applicable) ___________________________________________
Phone _____________ Address ________________________________________________
Have efforts been made to find a closer provider?
Is it medically necessary for this provider to treat this patient?
Yes Yes
No No
N/A
N/A
If the recipient has requested a special mode of transportation: |
|
|
|
Are there special transportation needs that you are aware of? |
Yes |
No |
N/A |
Please explain: _______________________________________________________________
Name of Physician completing form: ______________________ Phone ________________
Duration of need: From _____________ To _______________ |
OR |
Permanent
Physician’s Signature: _________________________________ Date _________________