The DMA 5048 form is a document that is used to apply for membership in the Direct Marketing Association. The form can be downloaded from the DMA website, and must be completed and submitted along with other required documentation. Membership in the DMA provides access to a variety of resources, including marketing research and education programs. Additionally, members have the opportunity to network with other professionals in the industry.
| Question | Answer |
|---|---|
| Form Name | Dma 5048 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form dma 5048, dma 5048 form, dma form 5048, dma5048 form |
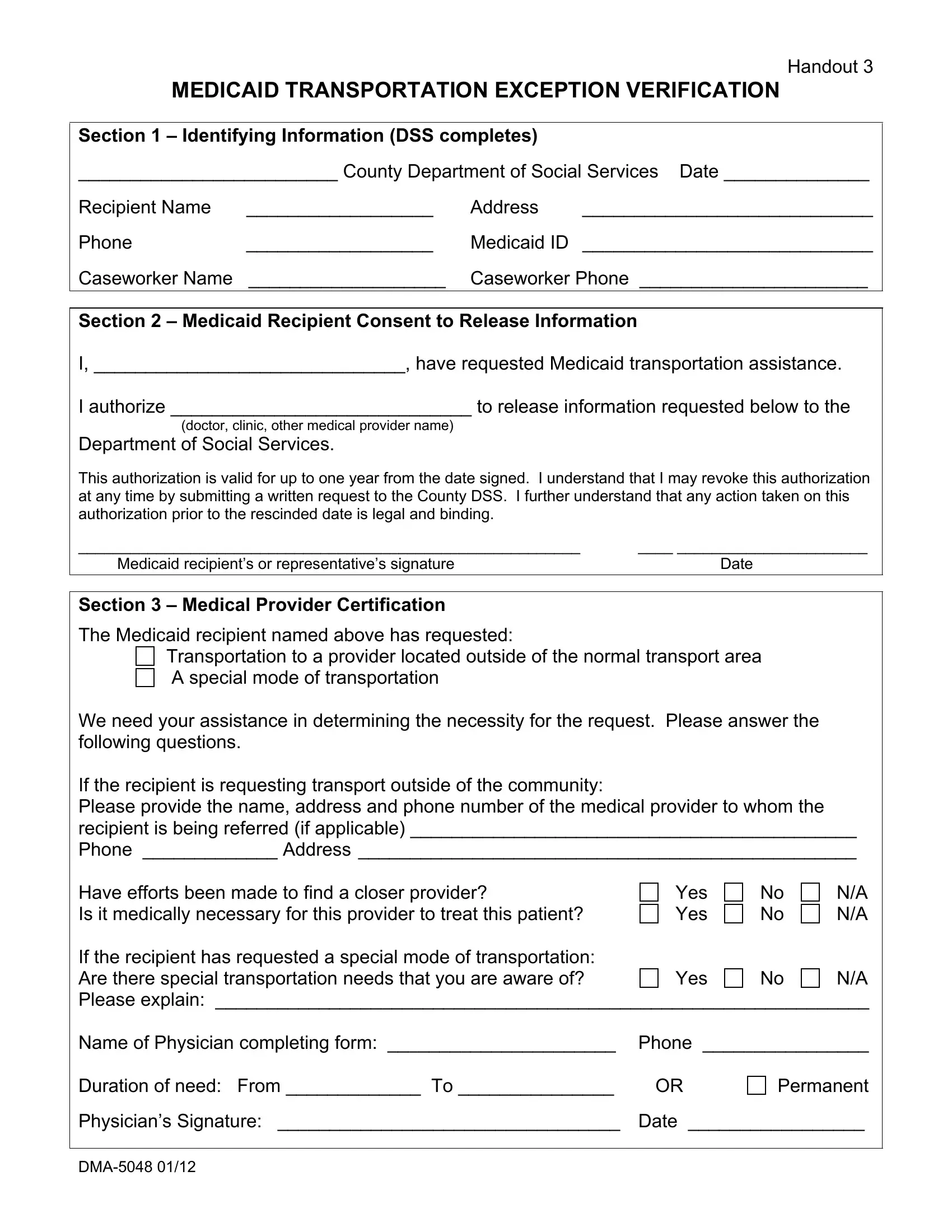
Handout 3
MEDICAID TRANSPORTATION EXCEPTION VERIFICATION
Section 1 – Identifying Information (DSS completes)
_________________________ County Department of Social Services Date ______________
Recipient Name |
__________________ |
Address |
____________________________ |
Phone |
__________________ |
Medicaid ID |
____________________________ |
Caseworker Name |
___________________ |
Caseworker Phone ______________________ |
|
Section 2 – Medicaid Recipient Consent to Release Information
I, ______________________________, have requested Medicaid transportation assistance.
I authorize _____________________________ to release information requested below to the
Department of Social Services.
This authorization is valid for up to one year from the date signed. I understand that I may revoke this authorization at any time by submitting a written request to the County DSS. I further understand that any action taken on this authorization prior to the rescinded date is legal and binding.
__________________________________________________________ |
____ ______________________ |
Medicaid recipient’s or representative’s signature |
Date |
Section 3 – Medical Provider Certification
The Medicaid recipient named above has requested:
Transportation to a provider located outside of the normal transport area A special mode of transportation
We need your assistance in determining the necessity for the request. Please answer the following questions.
If the recipient is requesting transport outside of the community:
Please provide the name, address and phone number of the medical provider to whom the recipient is being referred (if applicable) ___________________________________________
Phone _____________ Address ________________________________________________
Have efforts been made to find a closer provider?
Is it medically necessary for this provider to treat this patient?
Yes Yes
No No
N/A
N/A
If the recipient has requested a special mode of transportation: |
|
|
|
Are there special transportation needs that you are aware of? |
Yes |
No |
N/A |
Please explain: _______________________________________________________________
Name of Physician completing form: ______________________ Phone ________________
Duration of need: From _____________ To _______________ |
OR |
Permanent
Physician’s Signature: _________________________________ Date _________________