
With the help of the online editor for PDFs by FormsPal, you'll be able to fill out or modify yyyy right here and now. Our development team is continuously endeavoring to expand the tool and make it even faster for clients with its multiple functions. Enjoy an ever-evolving experience today! To get started on your journey, go through these simple steps:
Step 1: Click on the "Get Form" button in the top section of this page to open our editor.
Step 2: The editor helps you modify your PDF form in various ways. Transform it by adding customized text, correct what's originally in the PDF, and put in a signature - all readily available!
This document requires specific information to be entered, thus make sure to take whatever time to fill in exactly what is expected:
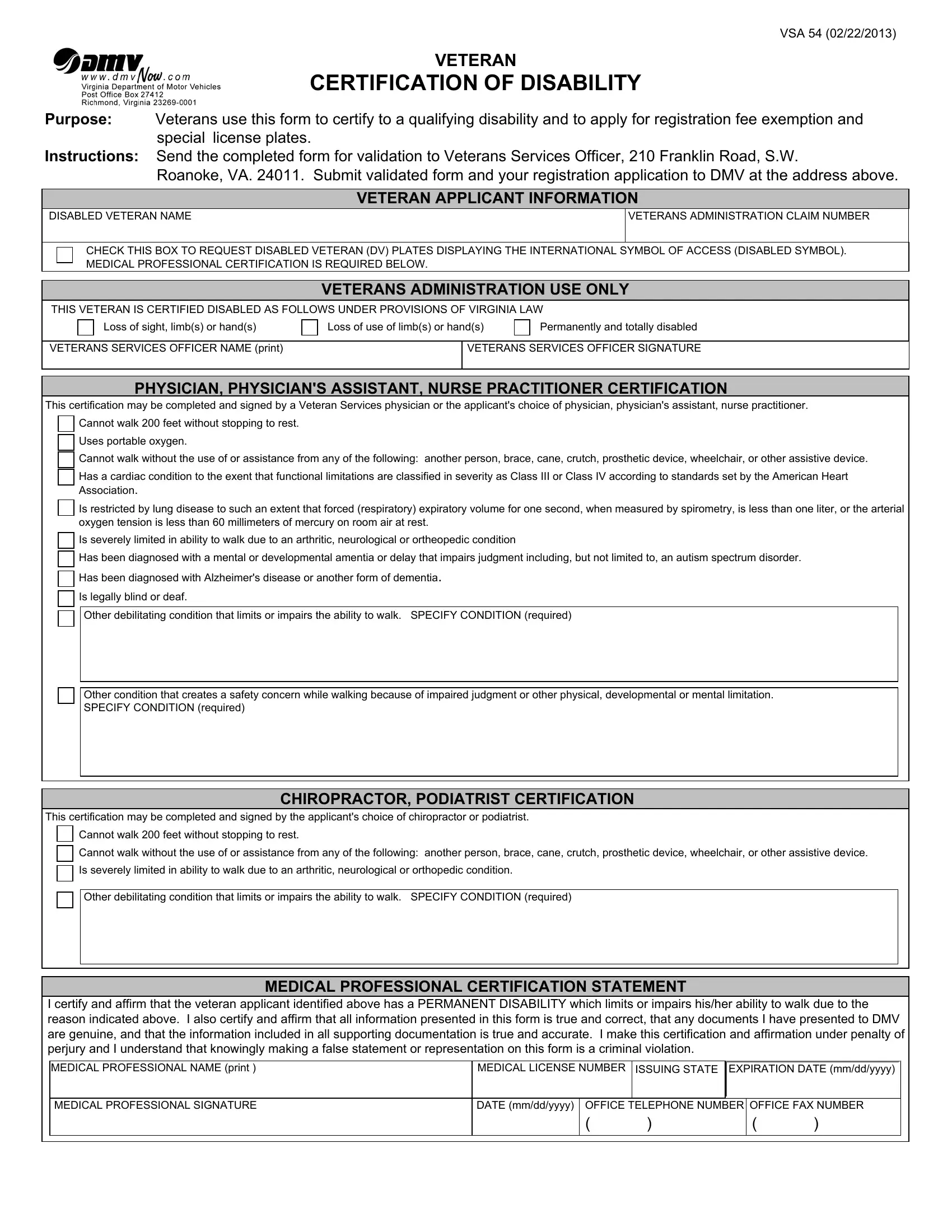
1. Complete the yyyy with a number of major fields. Consider all the necessary information and make certain there is nothing missed!
2. Once your current task is complete, take the next step – fill out all of these fields - Other condition that creates a, This certification may be, Cannot walk feet without stopping, CHIROPRACTOR PODIATRIST, Cannot walk without the use of or, Is severely limited in ability to, Other debilitating condition that, MEDICAL PROFESSIONAL CERTIFICATION, I certify and affirm that the, MEDICAL PROFESSIONAL NAME print, and MEDICAL LICENSE NUMBER ISSUING with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Be very attentive while filling in Cannot walk without the use of or and Is severely limited in ability to, as this is where a lot of people make a few mistakes.
Step 3: Check that your information is accurate and click on "Done" to proceed further. Create a 7-day free trial subscription with us and obtain direct access to yyyy - download or modify from your FormsPal account page. FormsPal ensures your information privacy by having a protected system that in no way saves or distributes any personal information typed in. Rest assured knowing your files are kept protected every time you work with our service!