
When you wish to fill out dmv critical need, it's not necessary to install any kind of programs - just give a try to our PDF editor. FormsPal team is focused on providing you with the perfect experience with our editor by regularly presenting new features and enhancements. With all of these improvements, using our editor becomes better than ever before! Here is what you'll want to do to get going:
Step 1: Just click on the "Get Form Button" above on this page to access our form editing tool. This way, you will find all that is required to work with your file.
Step 2: After you open the editor, you will notice the document all set to be filled in. In addition to filling out various blanks, you can also do many other things with the file, including adding any textual content, modifying the original text, inserting graphics, placing your signature to the document, and more.
This document requires specific information; in order to ensure accuracy, make sure you heed the guidelines directly below:
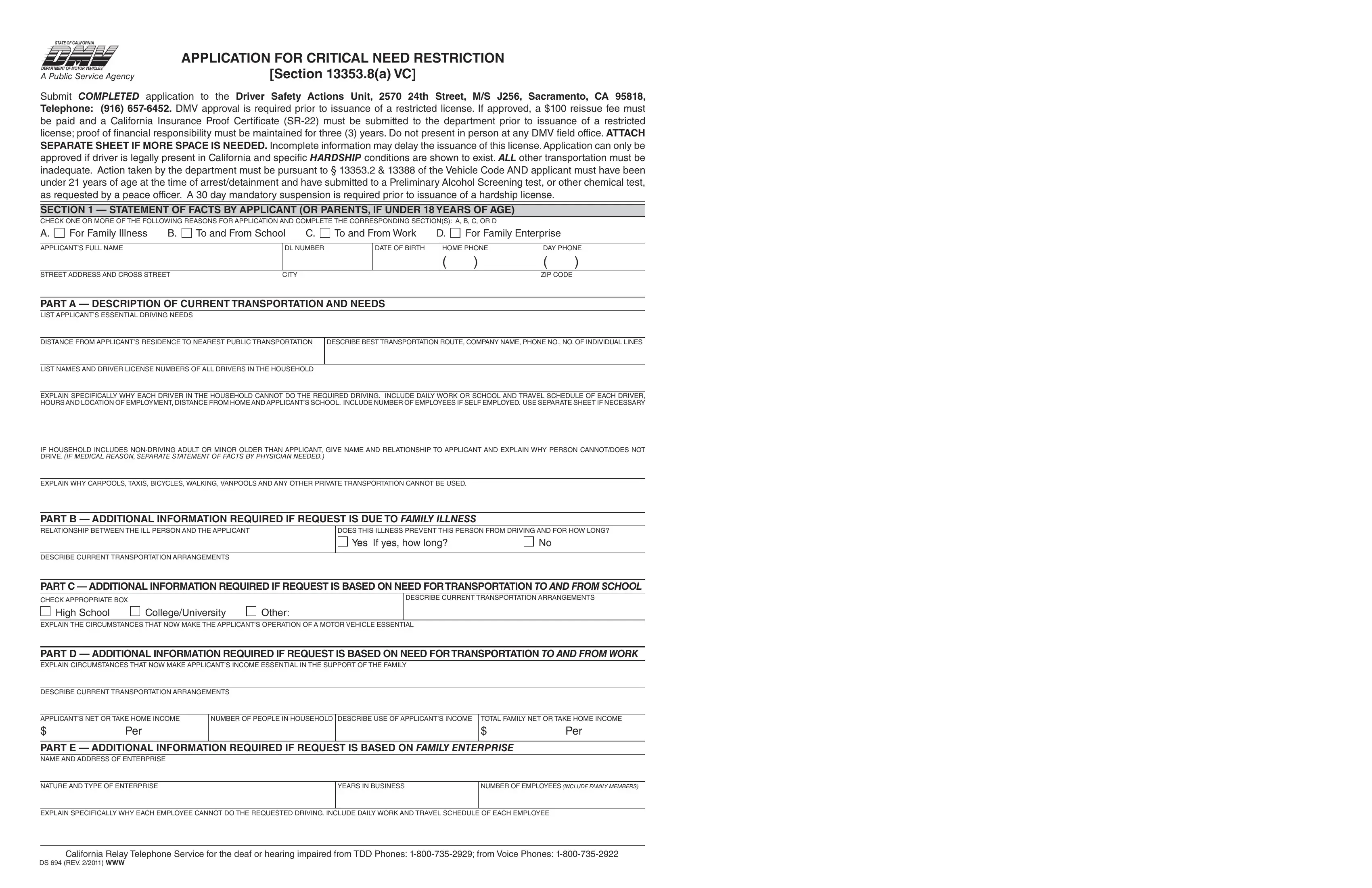
1. To start with, once filling out the dmv critical need, begin with the area with the subsequent blank fields:
2. The third step is usually to fill in the following fields: Yes If yes how long, DESCRIBE CURRENT TRANSPORTATION, PART C ADDITIONAL INFORMATION, CHECK APPROPRIATE BOX, High School, CollegeUniversity, Other, DESCRIBE CURRENT TRANSPORTATION, EXPLAIN THE CIRCUMSTANCES THAT NOW, PART D ADDITIONAL INFORMATION, DESCRIBE CURRENT TRANSPORTATION, APPLICANTS NET OR TAKE HOME INCOME, Per, NUMBER OF PEOPLE IN HOUSEHOLD, and Per.
3. Completing EXPLAIN WHY SOMEONE CANNOT BE, EXPLAIN WHY APPLICANTS OPERATION, HOURS PER WEEK APPLICANT WOULD WORK, SALARY IF ANY, AUTHORIZATION AND CERTIFICATION If, DIAGNOSIS, ADDRESS, ADDRESS, ADDRESS, ZIP CODE, ZIP CODE, ZIP CODE, DATE, CITY, and CITY is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
It is possible to get it wrong while filling out the CITY, for that reason you'll want to reread it before you finalize the form.
Step 3: Prior to moving on, you should make sure that form fields were filled in the right way. When you believe it's all fine, click on “Done." After creating a7-day free trial account here, you will be able to download dmv critical need or email it at once. The file will also be at your disposal from your personal account with your adjustments. FormsPal is committed to the privacy of all our users; we ensure that all information used in our editor stays protected.