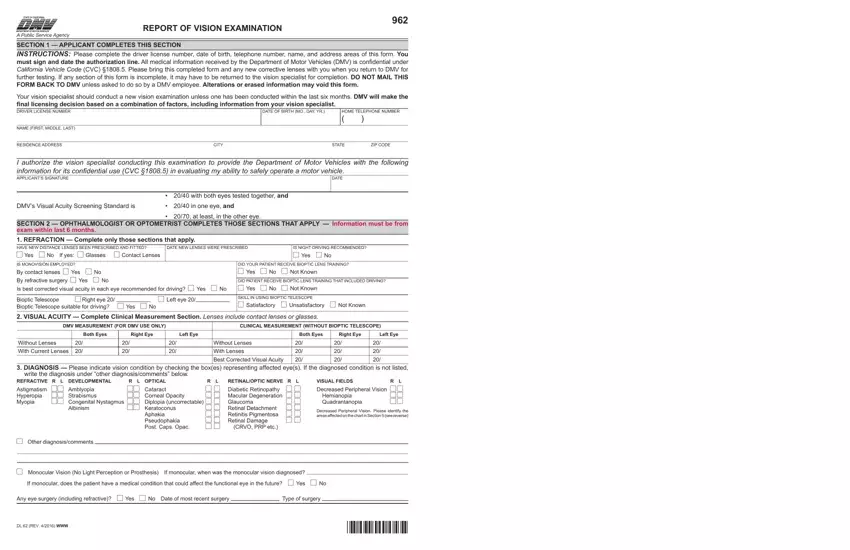
Navigating the roadways requires not only skill and knowledge of traffic laws but also adequate visual ability. In the State of California, the Department of Motor Vehicles (DMV) takes this aspect seriously, as evidenced by the DMV Vision Examination Report (Form 962). This critical form serves as a bridge between vision specialists and the DMV, ensuring drivers meet the necessary visual standards for safe driving. Divided into several sections, the form starts with the applicant’s contribution of personal details and an authorization signature that allows for their vision examination results to be used confidentially by the DMV. The onus then shifts to the ophthalmologist or optometrist, who fills in detailed information ranging from the prescription of new lenses, recommendations on night driving, and the employment of monovision or bioptic lenses. The form meticulously captures a plethora of data including clinical measurements of visual acuity with and without corrective lenses, diagnosis of specific vision conditions, prognosis, a thorough examination of visual fields, and additional observations about the patient’s vision that might affect their driving abilities. The form culminates with a physician's signature, which attests to the accuracy and validity of the examination findings. Overall, the DMV Vision Examination Report is crucial in making informed decisions about an individual’s fitness to drive, ensuring that the roads are safer for everyone.
| Question | Answer |
|---|---|
| Form Name | Dmv Vision Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dmv vision examination, ca dmv vision form, dmv ca gov form dl62, ca dmv form dl 62 |
