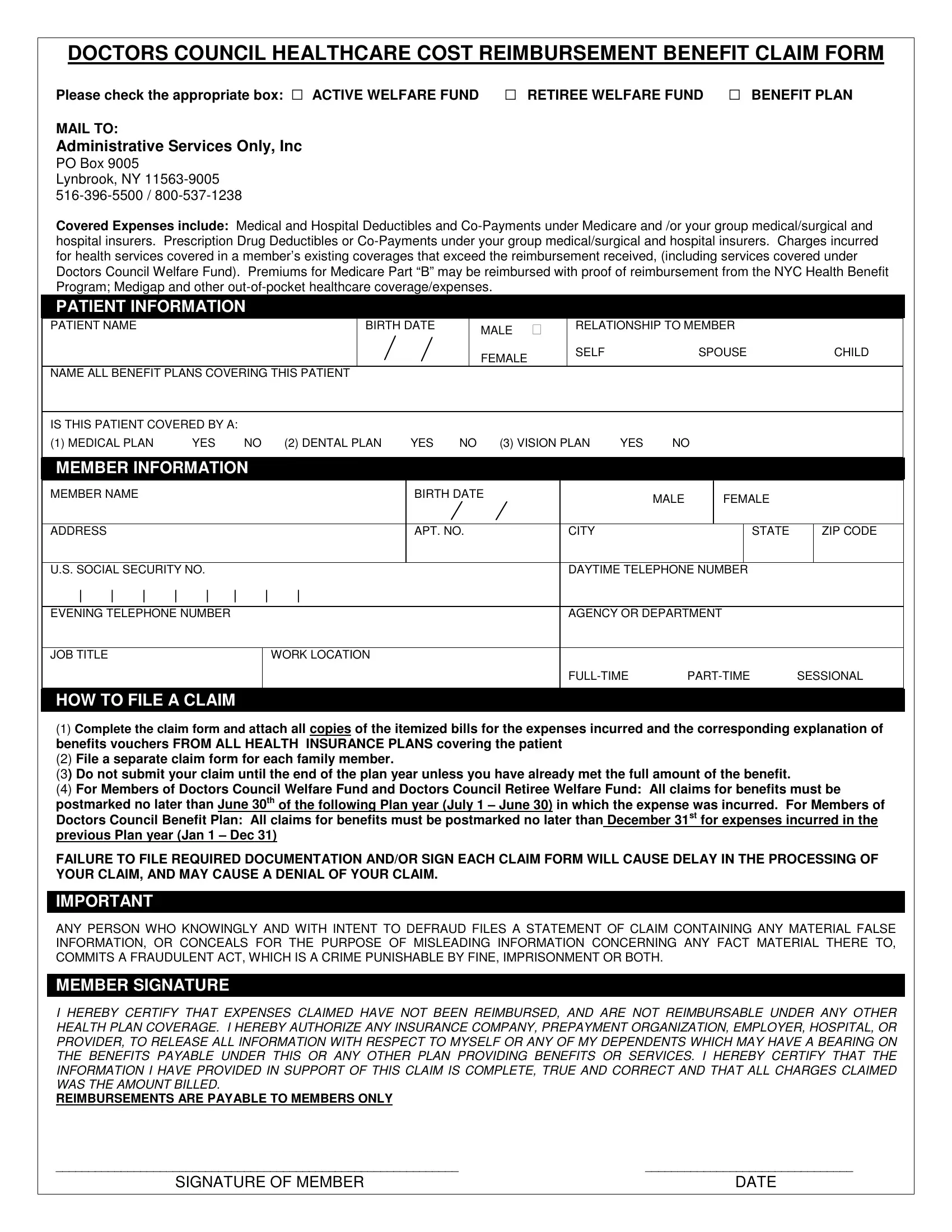
Filing for healthcare cost reimbursement showcases its own set of complexities, especially within specific plans like the Doctors Council Healthcare Cost Reimbursement Benefit Claim Form. This essential document caters to different categories of individuals, including those part of the Active Welfare Fund, the Retiree Welfare Fund, and the Benefit Plan, ensuring a smoother process for reclaiming medical, hospital, and prescription drug deductibles and co-payments. To submit a claim, the form requires detailed patient and member information, including health coverage specifics and identification data. Besides, patients must declare all applicable benefit plans and verify coverage under medical, dental, and vision plans. The submission guidelines are precise: complete the form, attach the necessary itemized bills and explanation of benefits, observe the deadline based on membership type, and ensure all submissions are accurately signed to avoid delays or denials. Notably, the form incorporates stern warnings against fraudulent claims, underscoring the legality and ethical considerations inherent in the process. The member's signature at the end of the form acts as a certification of the authenticity of the claim and an acknowledgment of the terms involved, reinforcing the serious nature of the claims process.
| Question | Answer |
|---|---|
| Form Name | Doctors Council Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | doctors council, 30th, doctor fill out sheet, doctor fill |
DOCTORS COUNCIL HEALTHCARE COST REIMBURSEMENT BENEFIT CLAIM FORM
Please check the appropriate box: ACTIVE WELFARE FUND RETIREE WELFARE FUND BENEFIT PLAN
MAIL TO:
Administrative Services Only, Inc
PO Box 9005
Lynbrook, NY
Covered Expenses include: Medical and Hospital Deductibles and
PATIENT INFORMATION
PATIENT NAME |
|
|
|
|
|
|
BIRTH DATE |
|
MALE |
RELATIONSHIP TO MEMBER |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
FEMALE |
SELF |
|
SPOUSE |
|
CHILD |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NAME ALL BENEFIT PLANS COVERING THIS PATIENT |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
IS THIS PATIENT COVERED BY A: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
(1) MEDICAL PLAN |
YES |
NO |
|
(2) DENTAL PLAN YES NO |
(3) VISION PLAN |
YES |
NO |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
MEMBER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
MEMBER NAME |
|
|
|
|
|
|
|
BIRTH DATE |
|
|
|
MALE |
|
FEMALE |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ADDRESS |
|
|
|
|
|
|
|
|
APT. NO. |
|
|
CITY |
|
|
|
|
|
STATE |
|
ZIP CODE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
U.S. SOCIAL SECURITY NO. |
|
|
|
|
|
|
|
|
DAYTIME TELEPHONE NUMBER |
|
|
|
|
|||||||||
| |
| |
| |
| |
| |
| |
| |
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
EVENING TELEPHONE NUMBER |
|
|
|
|
|
|
|
|
AGENCY OR DEPARTMENT |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
JOB TITLE |
|
|
|
|
|
|
WORK LOCATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
SESSIONAL |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOW TO FILE A CLAIM
(1)Complete the claim form and attach all copies of the itemized bills for the expenses incurred and the corresponding explanation of benefits vouchers FROM ALL HEALTH INSURANCE PLANS covering the patient
(2)File a separate claim form for each family member.
(3) Do not submit your claim until the end of the plan year unless you have already met the full amount of the benefit.
(4)For Members of Doctors Council Welfare Fund and Doctors Council Retiree Welfare Fund: All claims for benefits must be postmarked no later than June 30th of the following Plan year (July 1 – June 30) in which the expense was incurred. For Members of Doctors Council Benefit Plan: All claims for benefits must be postmarked no later than December 31st for expenses incurred in the previous Plan year (Jan 1 – Dec 31)
FAILURE TO FILE REQUIRED DOCUMENTATION AND/OR SIGN EACH CLAIM FORM WILL CAUSE DELAY IN THE PROCESSING OF YOUR CLAIM, AND MAY CAUSE A DENIAL OF YOUR CLAIM.
IMPORTANT
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD FILES A STATEMENT OF CLAIM CONTAINING ANY MATERIAL FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING INFORMATION CONCERNING ANY FACT MATERIAL THERE TO, COMMITS A FRAUDULENT ACT, WHICH IS A CRIME PUNISHABLE BY FINE, IMPRISONMENT OR BOTH.
MEMBER SIGNATURE
I HEREBY CERTIFY THAT EXPENSES CLAIMED HAVE NOT BEEN REIMBURSED, AND ARE NOT REIMBURSABLE UNDER ANY OTHER HEALTH PLAN COVERAGE. I HEREBY AUTHORIZE ANY INSURANCE COMPANY, PREPAYMENT ORGANIZATION, EMPLOYER, HOSPITAL, OR PROVIDER, TO RELEASE ALL INFORMATION WITH RESPECT TO MYSELF OR ANY OF MY DEPENDENTS WHICH MAY HAVE A BEARING ON THE BENEFITS PAYABLE UNDER THIS OR ANY OTHER PLAN PROVIDING BENEFITS OR SERVICES. I HEREBY CERTIFY THAT THE INFORMATION I HAVE PROVIDED IN SUPPORT OF THIS CLAIM IS COMPLETE, TRUE AND CORRECT AND THAT ALL CHARGES CLAIMED WAS THE AMOUNT BILLED.
REIMBURSEMENTS ARE PAYABLE TO MEMBERS ONLY
______________________________________________________________ |
________________________________ |
SIGNATURE OF MEMBER |
DATE |
|
|