

doh 1013 pdf can be filled in very easily. Simply open FormsPal PDF tool to get it done in a timely fashion. FormsPal team is relentlessly endeavoring to develop the editor and enable it to be much faster for clients with its many functions. Enjoy an ever-evolving experience now! With a few easy steps, it is possible to start your PDF editing:
Step 1: Press the "Get Form" button at the top of this page to access our PDF editor.
Step 2: After you launch the online editor, you'll see the document made ready to be completed. Other than filling in various blank fields, you may also perform some other things with the PDF, that is adding custom text, changing the initial text, inserting illustrations or photos, putting your signature on the form, and much more.
Be mindful while filling in this document. Make certain every single blank field is completed properly.
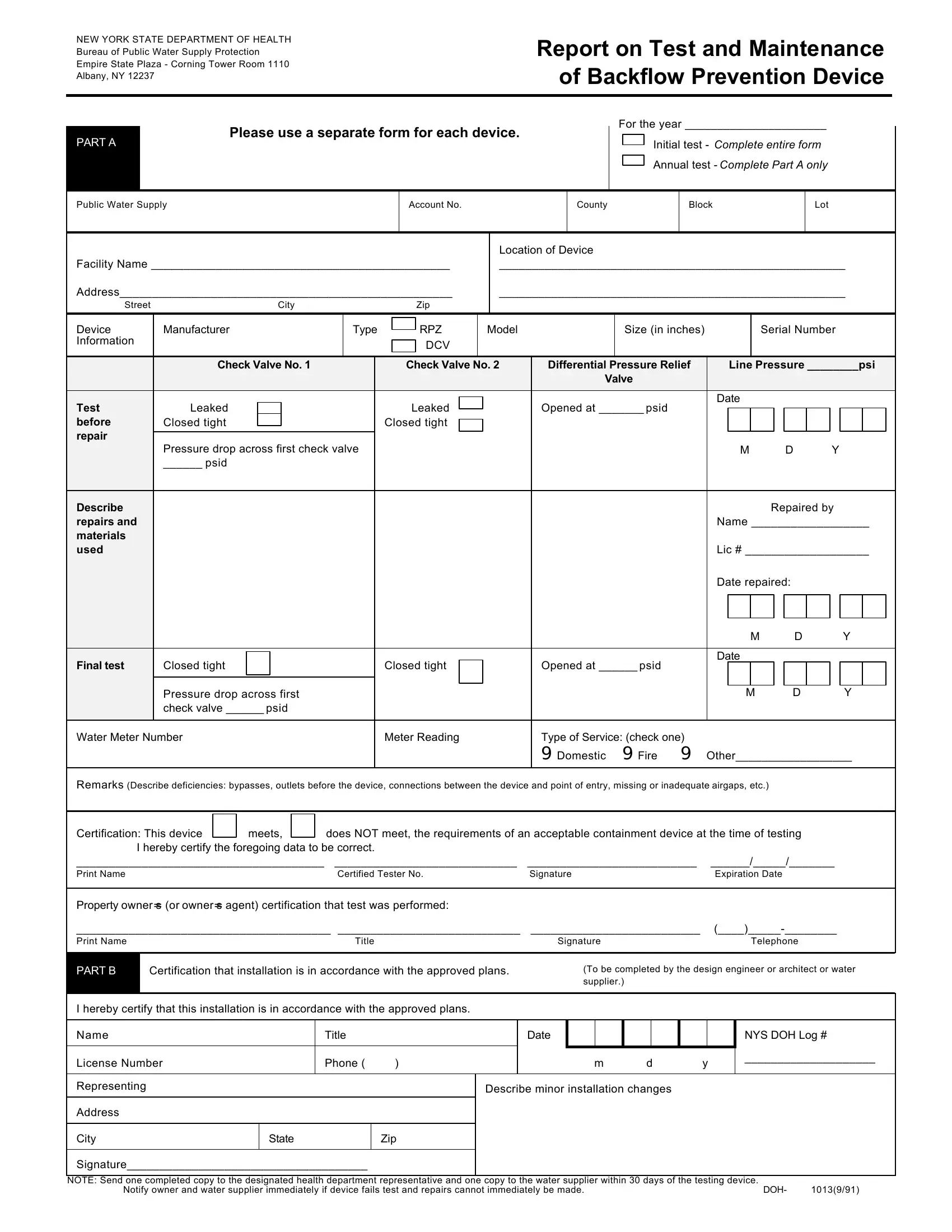
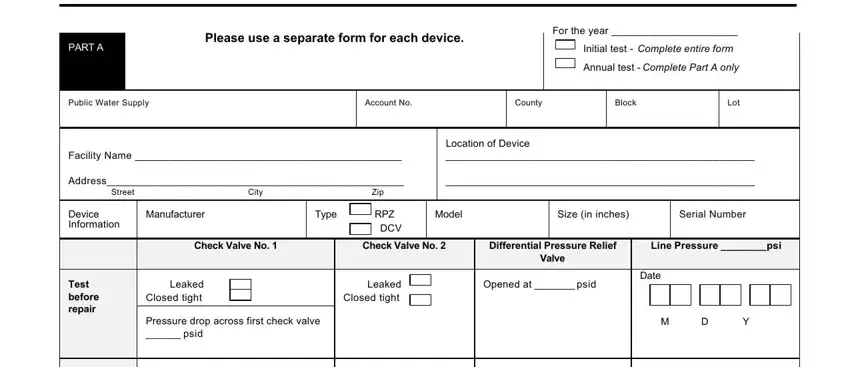
1. Fill out your doh 1013 pdf with a group of major fields. Collect all of the information you need and make sure absolutely nothing is left out!
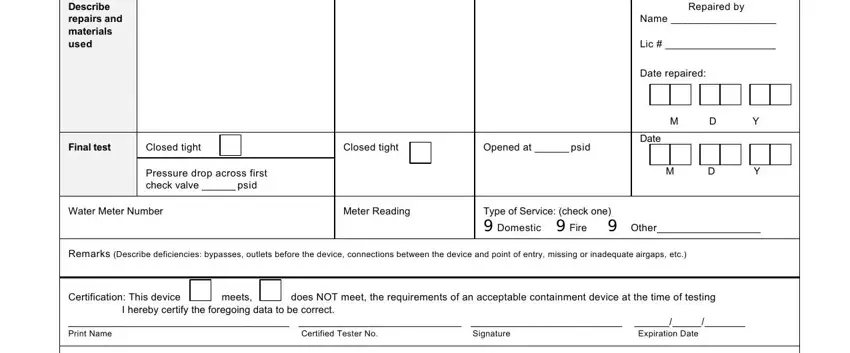
2. Once your current task is complete, take the next step – fill out all of these fields - Describe repairs and materials used, Repaired by, Name, Lic, Date repaired M D Y Date, M D Y, Final test, Closed tight, Closed tight, Opened at psid, Pressure drop across first check, Water Meter Number, Meter Reading, Type of Service check one, and Remarks Describe deficiencies with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this specific stage, have a look at Property owners or owners agent, PART B, Certification that installation is, To be completed by the design, I hereby certify that this, Name, License Number, Representing, Address, City, Title, Phone, Date, m d y, and Describe minor installation changes. Each of these will need to be filled out with utmost precision.
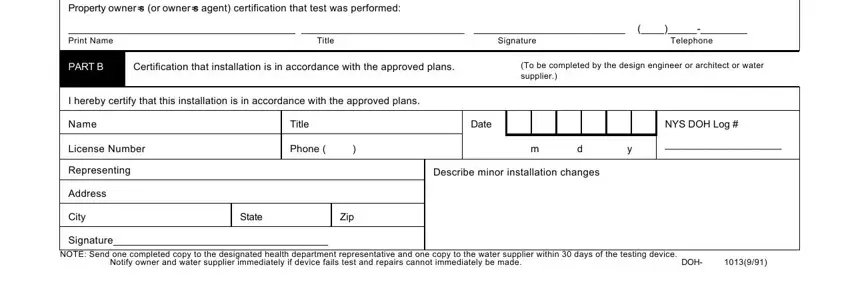
You can certainly make a mistake when completing the License Number, for that reason ensure that you reread it before you'll finalize the form.
Step 3: Ensure your details are accurate and click "Done" to progress further. Create a 7-day free trial account at FormsPal and obtain immediate access to doh 1013 pdf - which you may then work with as you want inside your personal cabinet. With FormsPal, you'll be able to fill out forms without being concerned about information breaches or records getting distributed. Our secure software makes sure that your personal details are maintained safe.