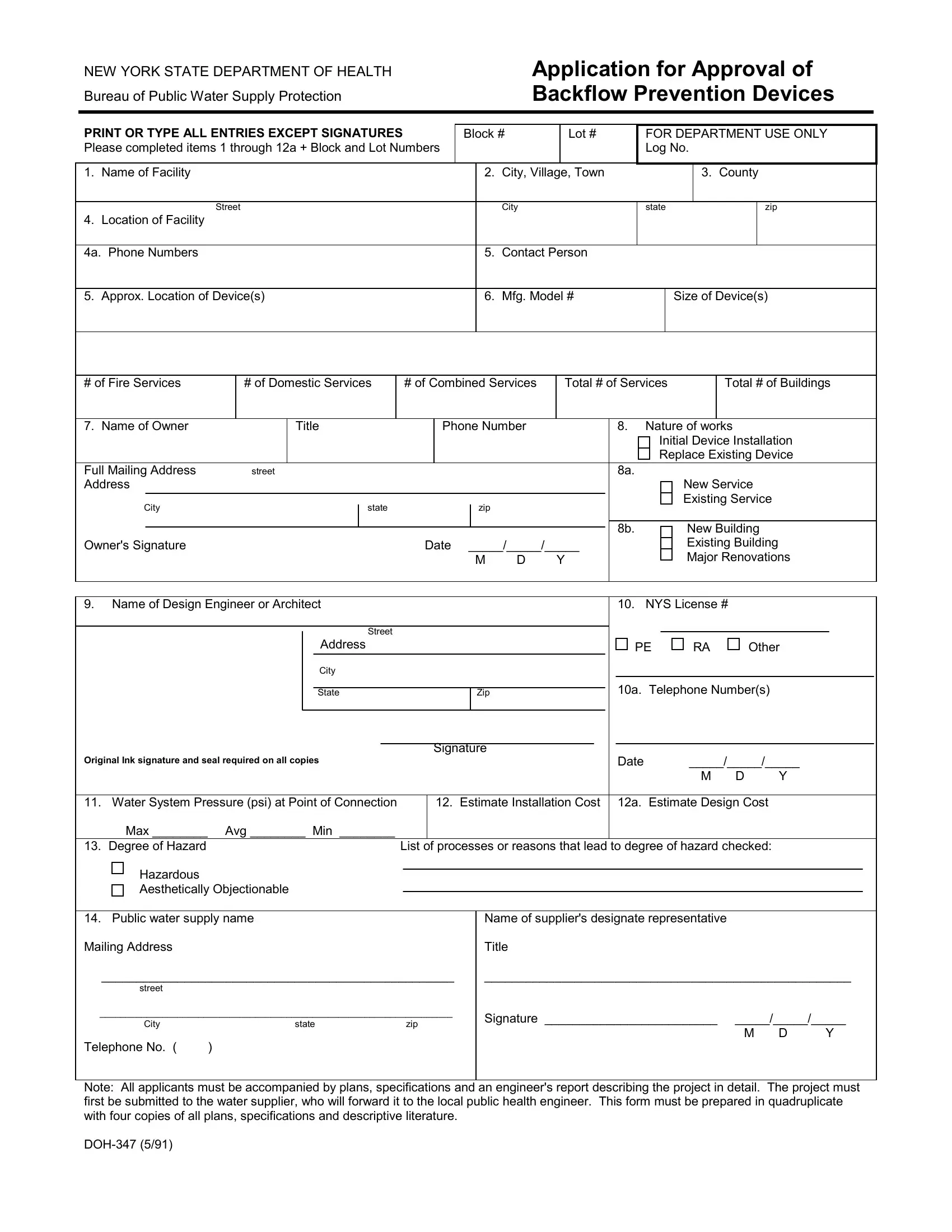
Ensuring the safety and integrity of public water supplies is a critical duty that falls upon various stakeholders, from local businesses to the New York State Department of Health. Within this context, the DOH-347 form serves as an essential instrument. This form, specifically designed by the Bureau of Public Water Supply Protection, is utilized to seek approval for the installation or replacement of backflow prevention devices. These devices are crucial in preventing contaminated water from flowing back into the public water system, thereby safeguarding the community's health. Applicants are required to provide comprehensive details, including the facility's name, location, and contact information, alongside technical specifics about the backflow prevention device such as the manufacturer, model number, and size. Additionally, the form delves into the nature of the installation—whether it pertains to a new service, a replacement, or major renovations—and requires information about the owner, design engineer or architect, and the estimated costs involved. The degree of hazard that the installation aims to mitigate is also a critical component, highlighting the significance of these devices in managing risks to the water supply. Plans, specifications, and an engineer’s report must accompany the form, emphasizing the thorough evaluation process undertaken to ensure compliance and safety. The DOH-347 form thus stands as a key document in the collaboration between business owners, engineers, and health departments to protect public health through the diligent management of water supply systems.
| Question | Answer |
|---|---|
| Form Name | Doh 347 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | doh 347 form, form doh 347, doh347, application backflow form |
NEW YORK STATE DEPARTMENT OF HEALTH
Bureau of Public Water Supply Protection
Application for Approval of Backflow Prevention Devices
PRINT OR TYPE ALL ENTRIES EXCEPT SIGNATURES |
Block # |
Lot # |
FOR DEPARTMENT USE ONLY |
|||||||
Please completed items 1 through 12a + Block and Lot Numbers |
|
|
|
|
Log No. |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
1. |
Name of Facility |
|
2. |
City, Village, Town |
|
|
3. |
County |
||
|
|
|
|
|
|
|
|
|
|
|
|
Street |
|
|
City |
|
state |
|
zip |
||
4. |
Location of Facility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
4a. Phone Numbers |
|
5. |
Contact Person |
|
|
|
|
|
||
|
|
|
|
|
|
|
||||
5. |
Approx. Location of Device(s) |
|
6. |
Mfg. Model # |
|
Size of Device(s) |
||||
|
|
|
|
|
|
|
|
|
|
|
# of Fire Services
# of Domestic Services
# of Combined Services
Total # of Services
Total # of Buildings
7. Name of Owner |
|
Title |
|
|
|
Phone Number |
|
|
|
8. |
|
Nature of works |
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initial Device Installation |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Replace Existing Device |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Full Mailing Address |
street |
|
|
|
|
|
|
|
|
|
|
|
|
8a. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New Service |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Existing Service |
|
|
|
|
|
||||
City |
|
|
|
|
state |
|
|
|
|
|
|
zip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8b. |
|
|
|
|
New Building |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Owner's Signature |
|
|
|
|
|
|
|
Date |
_____/_____/_____ |
|
|
|
|
|
|
|
|
|
|
Existing Building |
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
D |
Y |
|
|
|
|
|
|
|
|
Major Renovations |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
9. Name of Design Engineer or Architect |
|
|
|
|
|
|
|
|
|
|
|
10. |
|
NYS License # |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
PE |
|
|
RA |
|
|
Other |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10a. |
Telephone Number(s) |
|
|
|
|
|
|||||||||
|
|
|
|
|
State |
|
|
|
|
|
|
Zip |
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Original Ink signature and seal required on all copies |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
_____/_____/_____ |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
D |
Y |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
11. Water System Pressure (psi) at Point of Connection |
|
|
12. |
Estimate Installation Cost |
|
12a. |
Estimate Design Cost |
|
|
|
|
|
|||||||||||||||||||||||
Max ________ |
Avg ________ Min ________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
13. Degree of Hazard |
|
|
|
|
|
|
List of processes or reasons that lead to degree of hazard checked: |
|
|
|
|
|
|||||||||||||||||||||||
Hazardous |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Aesthetically Objectionable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
14. Public water supply name |
|
|
|
|
|
|
Name of supplier's designate representative |
|
|
|
|
|
|
|
|||||||||||||||||||||
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___________________________________________________ |
|
|
_____________________________________________________ |
|
|
||||||||||||||||||||||||||||||
street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____________________________________________________________________ |
|
|
Signature _________________________ |
_____/_____/_____ |
|
|
|||||||||||||||||||||||||||||
City |
|
state |
|
zip |
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
D |
Y |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Telephone No. ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Note: All applicants must be accompanied by plans, specifications and an engineer's report describing the project in detail. The project must first be submitted to the water supplier, who will forward it to the local public health engineer. This form must be prepared in quadruplicate with four copies of all plans, specifications and descriptive literature.