
Through the online PDF editor by FormsPal, it is possible to fill in or change new york state traveler form right here. Our tool is consistently developing to deliver the very best user experience possible, and that's because of our resolve for constant enhancement and listening closely to customer feedback. It merely requires just a few easy steps:
Step 1: Click the "Get Form" button above. It will open our editor so that you can start filling in your form.
Step 2: After you launch the online editor, there'll be the form prepared to be filled in. Aside from filling in different fields, you might also perform many other things with the file, specifically adding custom textual content, changing the initial text, inserting images, affixing your signature to the form, and much more.
It's straightforward to complete the document adhering to this practical guide! This is what you have to do:
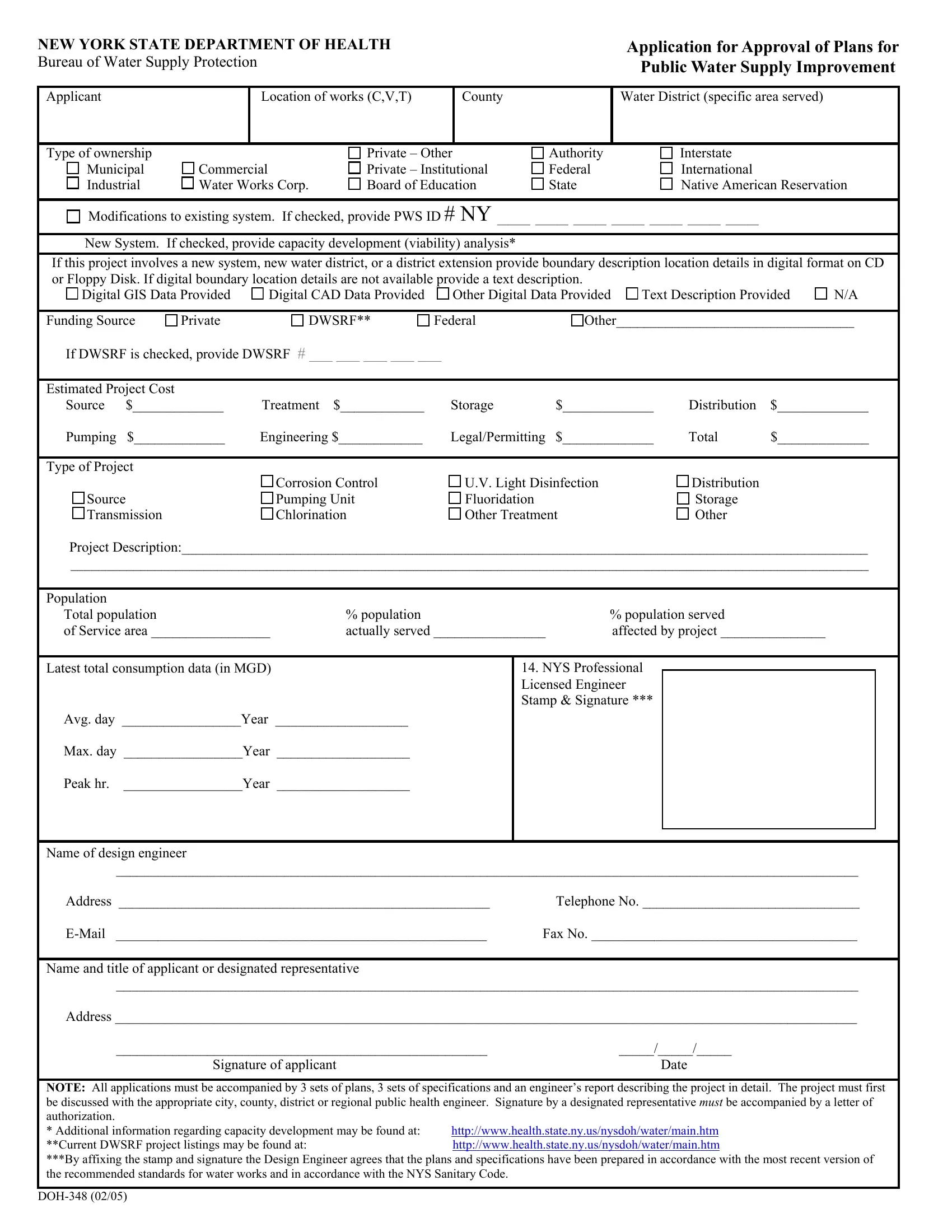
1. Begin filling out your new york state traveler form with a selection of essential fields. Gather all of the information you need and make certain absolutely nothing is missed!

Step 3: Check all the details you have typed into the blanks and click on the "Done" button. Create a 7-day free trial account with us and gain direct access to new york state traveler form - which you may then work with as you want inside your FormsPal cabinet. FormsPal guarantees secure form tools devoid of data recording or any sort of sharing. Rest assured that your information is in good hands here!