The notion regarding our PDF editor was to permit it to be as simple as it can be. You'll find the complete process of creating doh 4328 form trouble-free in the event you use these steps.
Step 1: The first thing is to click the orange "Get Form Now" button.
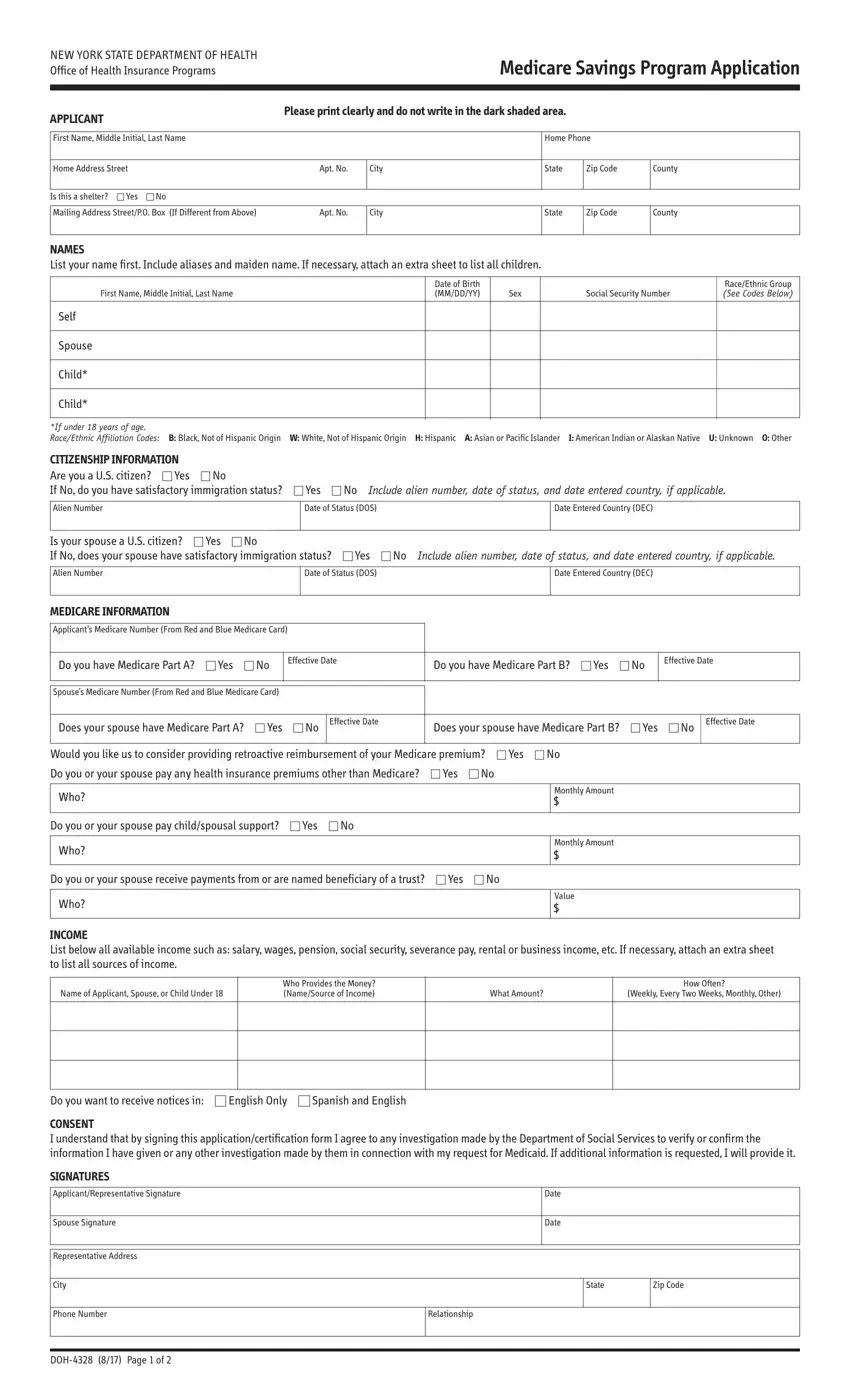
Step 2: So, you can begin editing the doh 4328 form. Our multifunctional toolbar is readily available - add, erase, adjust, highlight, and perform similar commands with the text in the form.
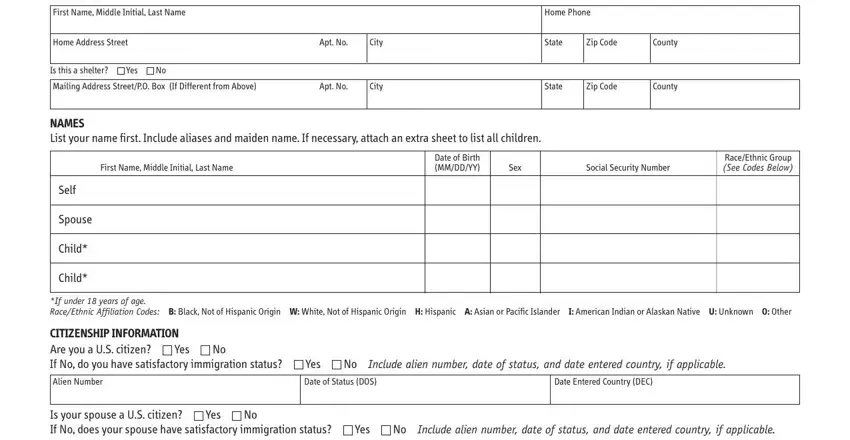
The PDF document you desire to create will cover the following sections:
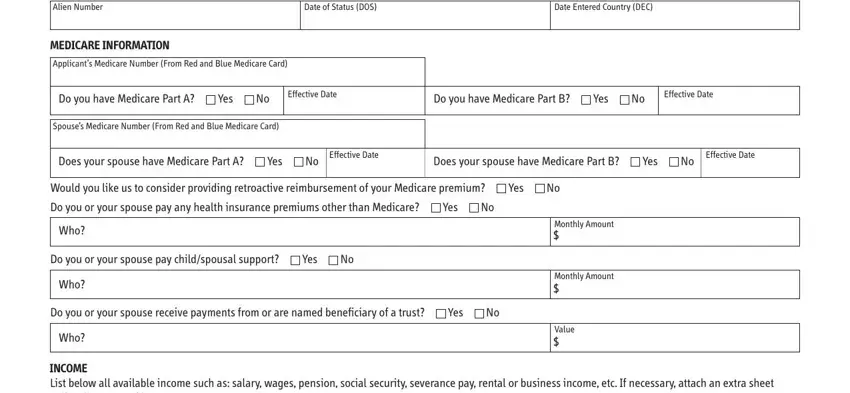
Fill out the Alien Number, Date of Status DOS, Date Entered Country DEC, MEDICARE INFORMATION, Applicants Medicare Number From, Do you have Medicare Part A, Yes, Effective Date, Do you have Medicare Part B, Yes, Effective Date, Spouses Medicare Number From Red, Does your spouse have Medicare, Yes, and Effective Date space with all the data asked by the software.
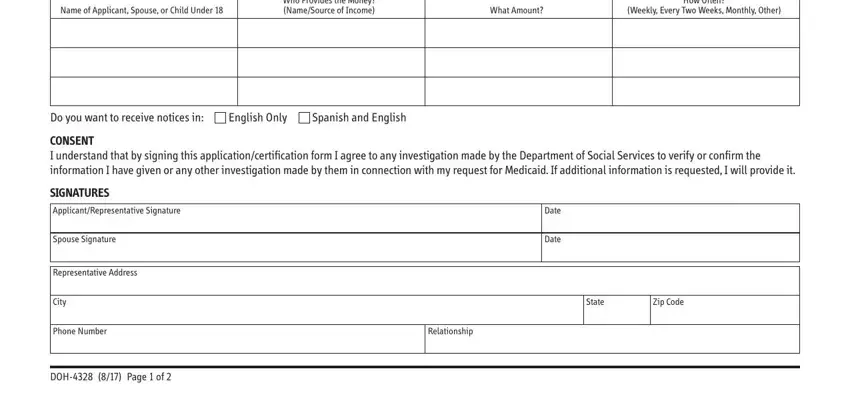
The software will require you to provide specific vital particulars to instantly fill in the section Name of Applicant Spouse or Child, Who Provides the Money NameSource, What Amount, How Often Weekly Every Two Weeks, Do you want to receive notices in, English Only, Spanish and English, CONSENT I understand that by, SIGNATURES ApplicantRepresentative, Spouse Signature, Representative Address, City, Phone Number, DOH Page of, and Date.
It is important to spell out the rights and responsibilities of both parties in section I consent to withdraw my, Applicant Signature, Date, Signature of Person Who Obtained, Date, Employed By, Date Eligibility Determined By, Date Eligibility Approved By, CentralOffice, Application Date, Unit ID, Worker ID, Case Type, Case No, and Reuse Ind.
Step 3: Once you have hit the Done button, your file is going to be readily available export to any type of electronic device or email you indicate.
Step 4: You can make duplicates of your form toavoid all of the potential issues. Don't worry, we cannot display or watch your data.
