Our top level web developers worked hard to build the PDF editor we are extremely pleased to deliver to you. Our software makes it possible to easily create cdpap form 2020 pdf and will save you precious time. You just need to try out this particular procedure.
Step 1: Press the button "Get form here" to access it.
Step 2: So you're on the document editing page. You can change and add text to the document, highlight words and phrases, cross or check particular words, include images, put a signature on it, delete needless areas, or remove them completely.
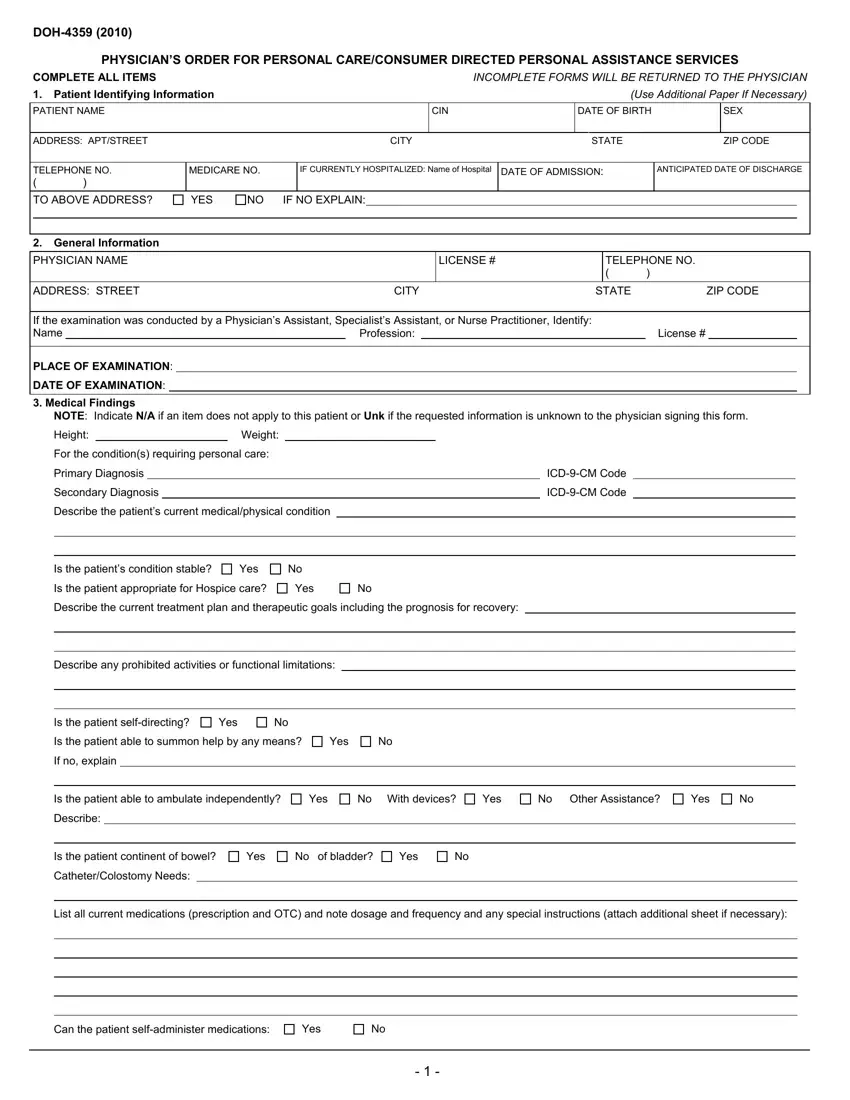
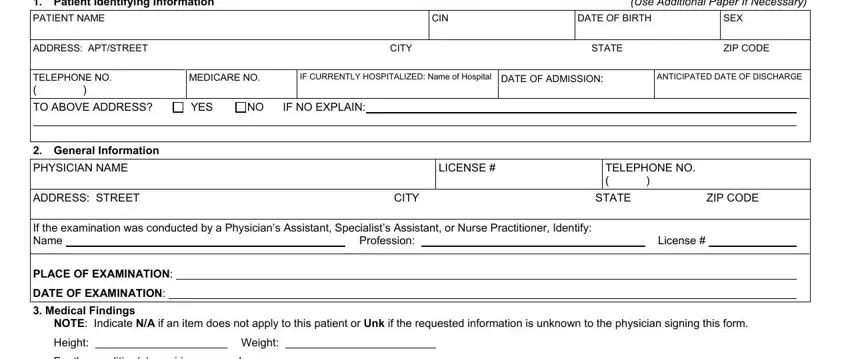
You have to type in the following data in order to complete the file:
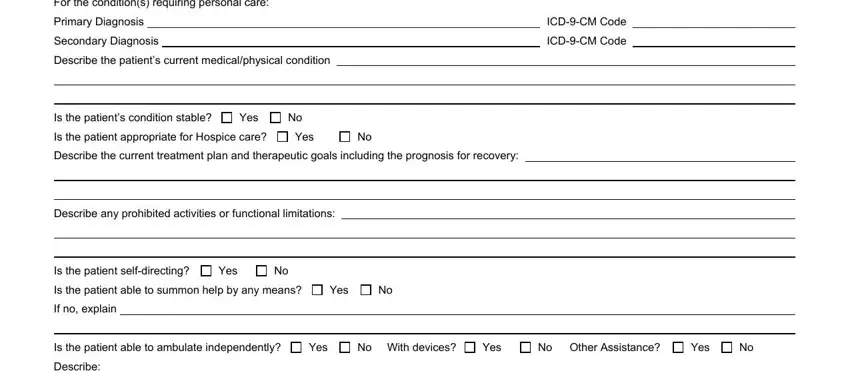
Type in the information in the For the conditions requiring, Primary Diagnosis, Secondary Diagnosis, Describe the patients current, ICDCM Code, ICDCM Code, Is the patients condition stable, Yes, Is the patient appropriate for, Yes, Describe the current treatment, Describe any prohibited activities, Is the patient selfdirecting, Yes, and Is the patient able to summon help field.
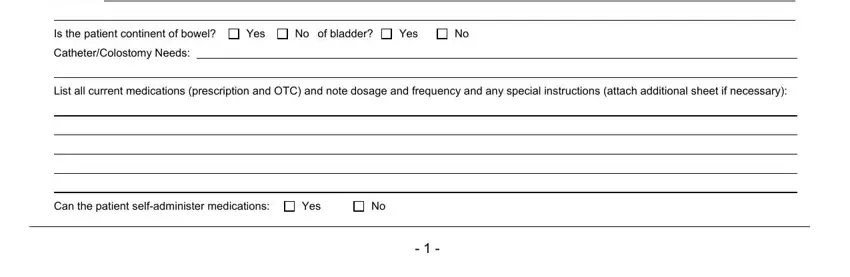
Be sure to point out the relevant particulars within the Describe, Is the patient continent of bowel, Yes, No of bladder, Yes, CatheterColostomy Needs, List all current medications, Can the patient selfadminister, and Yes section.
The If the patient requires a modified, Please indicate any task, Does the patient require, Yes, If Yes please indicate, Based on the medical condition do, Yes, Contributing Factors, Describe contributing factors, decreased stamina etc situation, for assistance with skilled tasks, and assistance with home care services box could be used to indicate the rights and responsibilities of either side.
Fill in the template by reading all these areas: assistance with home care services, IT IS MY OPINION THAT THIS PATIENT, and INCOMPLETE OR MISSING INFORMATION.
Step 3: If you are done, hit the "Done" button to transfer your PDF document.
Step 4: Ensure that you stay away from possible future challenges by getting no less than two duplicates of your document.
