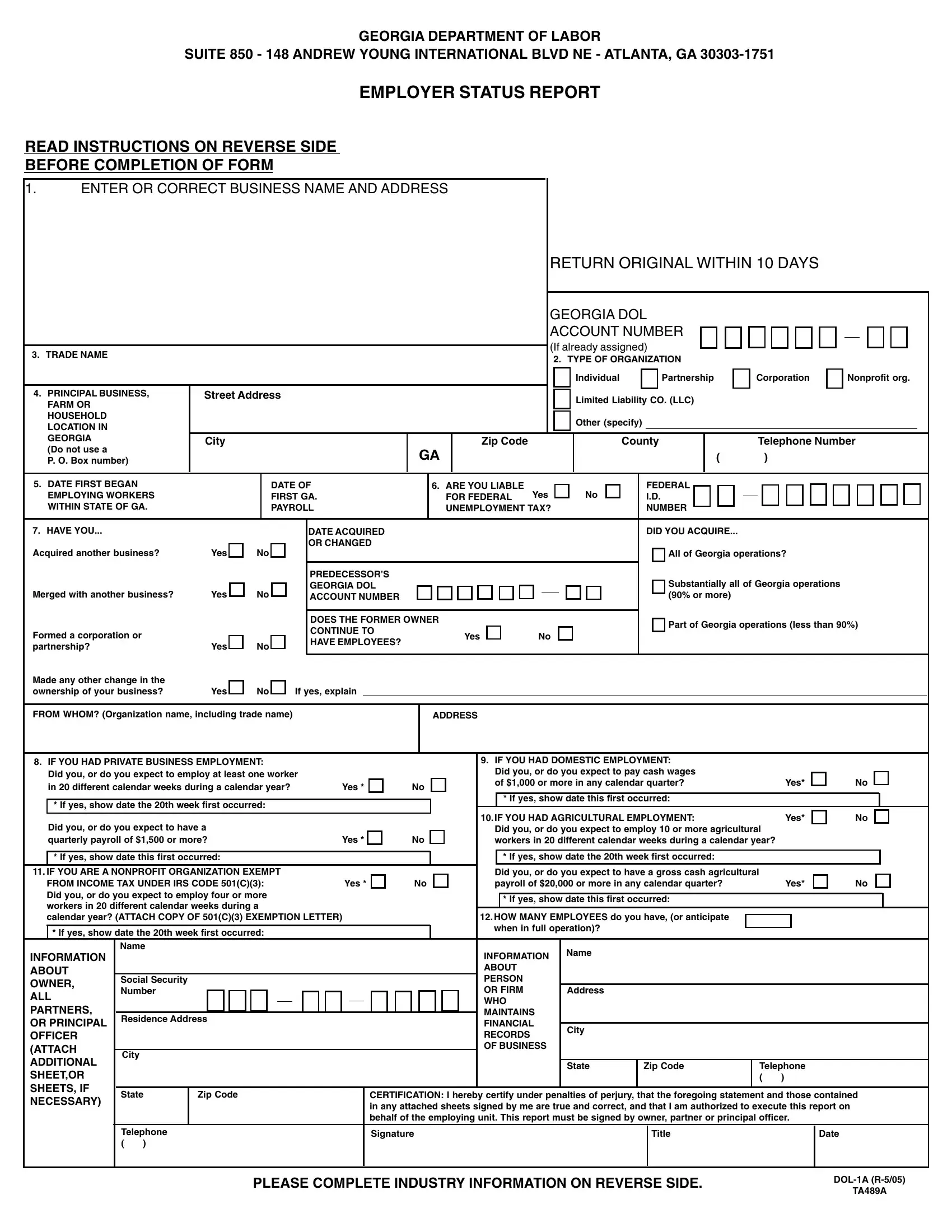
Initiating a business in Georgia involves various steps, among which a significant early task is completing the Department of Labor 1A Form, commonly known as the Employer Status Report. This critical form serves multiple functions: it helps determine an employer's liability for federal unemployment tax, facilitates the assignment of a Georgia Department of Labor Account Number, and gathers specific information about the business, including but not limited to the type of organization (e.g., individual, partnership, corporation), trade name, primary business location, and the nature of the business activities. Additionally, the form addresses various employment situations, querying whether the employer has engaged in private, agricultural, domestic employment, or operates as a nonprofit organization. This comprehensive approach not only aids in classifying the business for state labor records but also in ensuring compliance with state law regarding employment and payroll. Employers are prompted to provide detailed information about their operation, including the date they began employing workers in Georgia, if and when they acquired another business, and projections on employee numbers. The nuanced details requested underscore the form's importance in establishing a new or acquired business's legal and operational framework within the state.
| Question | Answer |
|---|---|
| Form Name | Dol 1A Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | SHEETOR, DOL-1, exempting, R-5 |
GEORGIA DEPARTMENT OF LABOR
SUITE 850 - 148 ANDREW YOUNG INTERNATIONAL BLVD NE - ATLANTA, GA
EMPLOYER STATUS REPORT
READ INSTRUCTIONS ON REVERSE SIDE
BEFORE COMPLETION OF FORM
1.ENTER OR CORRECT BUSINESS NAME AND ADDRESS
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RETURN ORIGINAL WITHIN 10 DAYS |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GEORGIA DOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCOUNT NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(If already assigned) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
3. TRADE NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. TYPE OF ORGANIZATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Individual |
|
|
|
Partnership |
|
|
Corporation |
|
|
Nonprofit org. |
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
4. PRINCIPAL BUSINESS, |
Street Address |
|
|
|
|
|
|
|
|
|
|
|
Limited Liability CO. (LLC) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
FARM OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOUSEHOLD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
LOCATION IN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GEORGIA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
County |
|
|
|
|
Telephone Number |
|
|
|
||||||||||||||||||||||||||||
(Do not use a |
|
|
|
|
|
|
GA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
P. O. Box number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
5. DATE FIRST BEGAN |
|
|
|
DATE OF |
|
6. ARE YOU LIABLE |
Yes |
|
|
|
|
No |
|
|
FEDERAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
EMPLOYING WORKERS |
|
|
|
FIRST GA. |
|
FOR FEDERAL |
|
|
|
|
|
|
I.D. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
WITHIN STATE OF GA. |
|
|
|
PAYROLL |
|
UNEMPLOYMENT TAX? |
|
|
NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
7. HAVE YOU... |
|
|
|
|
DATE ACQUIRED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DID YOU ACQUIRE... |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
OR CHANGED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Acquired another business? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All of Georgia operations? |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREDECESSOR’S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Merged with another business? |
Yes |
No |
|
GEORGIA DOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Substantially all of Georgia operations |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
ACCOUNT NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(90% or more) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
DOES THE FORMER OWNER |
|
|
|
|
|
|
|
|
|
|
|
|
Part of Georgia operations (less than 90%) |
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
CONTINUE TO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
Formed a corporation or |
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
HAVE EMPLOYEES? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
partnership? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Made any other change in the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ownership of your business? |
Yes |
No |
If yes, explain |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
FROM WHOM? (Organization name, including trade name)
ADDRESS
8. IF YOU HAD PRIVATE BUSINESS EMPLOYMENT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. IF YOU HAD DOMESTIC EMPLOYMENT: |
|
|
|
|
|
|
||||||||||||||||||
|
Did you, or do you expect to employ at least one worker |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Did you, or do you expect to pay cash wages |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of $1,000 or more in any calendar quarter? |
|
Yes* |
No |
|||||||||||||||||||||
|
in 20 different calendar weeks during a calendar year? |
|
|
|
Yes * |
|
|
|
No |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
* If yes, show date the 20th week first occurred: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* If yes, show date this first occurred: |
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. IF YOU HAD AGRICULTURAL EMPLOYMENT: |
|
Yes* |
No |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Did you, or do you expect to have a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Did you, or do you expect to employ 10 or more agricultural |
|
|
|
|
|
||||||||||||||||||
|
quarterly payroll of $1,500 or more? |
|
|
|
Yes * |
|
|
|
No |
workers in 20 different calendar weeks during a calendar year? |
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
* If yes, show date this first occurred: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* If yes, show date the 20th week first occurred: |
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. IF YOU ARE A NONPROFIT ORGANIZATION EXEMPT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Did you, or do you expect to have a gross cash agricultural |
|
|
|
|
|
|
||||||||||||||||||
|
FROM INCOME TAX UNDER IRS CODE 501(C)(3): |
|
|
|
Yes * |
|
|
|
No |
payroll of $20,000 or more in any calendar quarter? |
|
Yes* |
No |
|||||||||||||||||||||||||||
|
Did you, or do you expect to employ four or more |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* If yes, show date this first occurred: |
|
|
|
|
|
|
|||||||||||||||||
|
workers in 20 different calendar weeks during a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
calendar year? (ATTACH COPY OF 501(C)(3) EXEMPTION LETTER) |
|
|
|
|
|
|
|
|
|
12. HOW MANY EMPLOYEES do you have, (or anticipate |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
* If yes, show date the 20th week first occurred: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
when in full operation)? |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
ABOUT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ABOUT |
|
|
|
|
|
|
|
|
|
|
|
|||
OWNER, |
Social Security |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PERSON |
|
|
|
|
|
|
|
|
|
|
|
|||
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OR FIRM |
Address |
|
|
|
|
|
|
|
|
|
|
||||
ALL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WHO |
|
|
|
|
|
|
|
|
|
|
|
||||
PARTNERS, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MAINTAINS |
|
|
|
|
|
|
|
|
|
|
|
||||
Residence Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
OR PRINCIPAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FINANCIAL |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|||||
OFFICER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECORDS |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
(ATTACH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF BUSINESS |
|
|
|
|
|
|
|
|
|
|
|
|||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ADDITIONAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
Zip Code |
|
Telephone |
|
|
||||||||
SHEET,OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|||
SHEETS, IF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
State |
Zip Code |
|
|
|
|
|
|
CERTIFICATION: I hereby certify under penalties of perjury, that the foregoing statement and those contained |
||||||||||||||||||||||||||||||||
NECESSARY) |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
in any attached sheets signed by me are true and correct, and that I am authorized to execute this report on |
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
behalf of the employing unit. This report must be signed by owner, partner or principal officer. |
|
|
|||||||||||||||||||
|
|
|
Telephone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature |
|
|
|
|
Title |
|
|
|
Date |
|
|
||||||||||
|
|
|
( ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE COMPLETE INDUSTRY INFORMATION ON REVERSE SIDE.
TA489A