Completion |
|
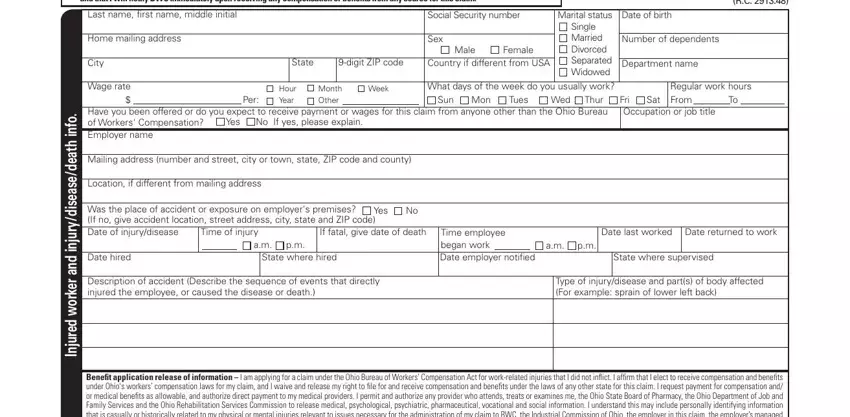
Last name, first name, middle initial |
|
|
|
|
|
|
|
Social Security number |
|
Marital status |
|
Date of birth |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
|
|
|
|
|
|
|
|
|
|
instructions |
info. |
Home mailing address |
1 |
|
|
|
|
|
|
|
|
|
Sex |
|
|
|
|
Married |
|
Number of dependents |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
Female |
Divorced |
|
|
|
|
|
|
|
|
|
|
|
|
(continued) |
|
City |
|
|
|
|
|
|
State |
|
9-digit ZIP code |
Country if different from USA |
Separated |
|
Department name |
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Widowed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
injury/disease/death |
Wage rate |
|
|
|
|
Hour |
Month |
Week |
What days of the week do you usually work? |
|
|
|
Regular work hours |
|
|
|
|
|
|
|
|
$________________ Per: 3 |
Year |
Other _________________ |
4 |
|
Sun |
Mon |
Tues |
Wed |
Thur |
|
Fri |
Sat |
From ____ To ____ 4 |
|
|
|
|
|
|
|
Have you been offered or do you expect to receive payment or wages for this claim from anyone other than the Ohio Bureau |
5 |
|
|
|
|
Occupation or job title |
6 |
|
|
|
|
|
|
|
|
|
of Workers' Compensation? YES |
NO If yes, please explain. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer name |
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street, city or town, state, ZIP code and county) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Location, if different from mailing address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Was place of accident or exposure on employer's premises? Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If no, give accident location, street address, city, state and ZIP code. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of injury/disease |
8 |
Time of injury |
|
|
If fatal, give date of death |
|
Time employee began |
Date last worked |
9 |
Date returned to work |
|
|
|
|
|
|
|
|
|
|
__________ |
|
a.m. |
p.m. |
|
|
|
|
|
|
work |
a.m. |
p.m. |
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
Date hired |
|
|
|
State where hired |
11 |
|
|
|
Date employer notified 12 |
State where supervised |
13 |
|
|
|
|
|
|
|
|
|
|
|
|
|
and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Description of accident (Describe the sequence of events that directly |
14 |
|
|
|
|
|
|
|
Type of injury/disease and part(s) of body affected |
|
|
|
|
|
|
|
|
injured the employee, or caused the disease or death) |
|
|
|
|
|
|
|
|
|
|
|
(for example: sprain of lower left back, etc.) |
|
15 |
|
|
|
|
|
|
|
|
worker |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
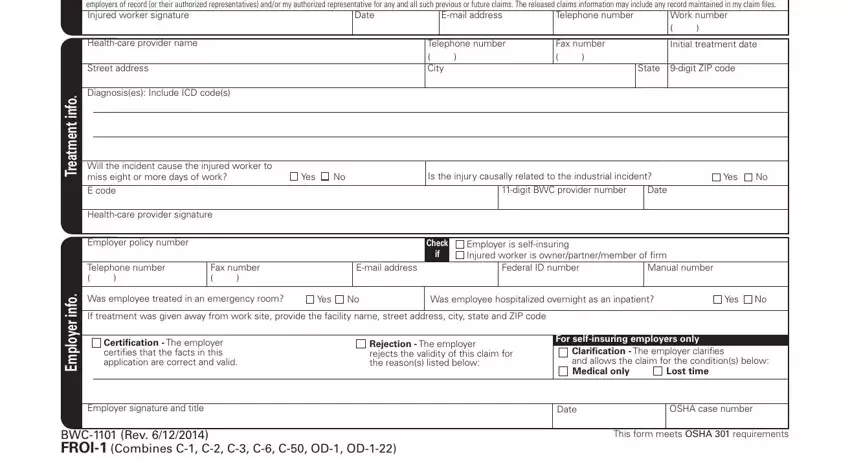
Benefit application release of information – I am applying for a claim under the Ohio Bureau of Workers’ Compensation Act for work-related injuries that I did not inflict. I affirm that I elect to receive compensation |
|
|
|
|
|
|
|
|
and benefits under Ohio's workers’ compensation laws for my claim, and I waive and release my right to file for and receive compensation and benefits under the laws of any other state for this claim. I request |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Injured |
payment for compensation and/or medical benefits as allowable, and authorize direct payment to my medical providers. I permit and authorize any provider who attends, treats or examines me, the Ohio State Board |
|
|
|
|
|
|
|
|
of Pharmacy, the Ohio Department of Job and Family Services and the Ohio Rehabilitation Services Commission to release medical, psychological, psychiatric, pharmaceutical, vocational and social information. I |
|
|
|
|
|
|
|
|
understand this may include personally identifying information that is casually or historically related to my physical or mental injuries relevant to issues necessary for the administration of my claim to BWC, the |
|
|
|
|
|
|
|
|
Industrial Commission of Ohio, the employer in this claim, the employer’s managed care organization and any authorized representatives. My previous or future BWC claims may affect decisions made in this claim. |
|
|
|
|
|
|
|
|
Proper administration of the present claim may require BWC to share claims information with the employers of record (or their authorized representatives) and/or my authorized representative for any and all such |
|
|
|
|
|
|
|
|
|
previous or future claims. The released claims information may include any record maintained in my claim files. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Injured worker signature |
16 |
|
|
|
|
|
|
Date |
|
|
|
E-mail address |
|
|
Telephone number |
Work number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( ) |
|
|
|
( ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 Home address: Enter the home address where the |
|
9 Date last worked: Enter the last day worked as a result |
|
|
|
|
injured worker lives. Include the apartment number, |
|
|
|
of this injury, occupational disease or death. |
|
|
|
|
if applicable. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• If the post ofice does not deliver mail to the |
10 |
|
Date returned to work: Enter the date the injured |
|
|
|
|
|
home address, list the mailing address instead |
|
|
|
worker returned to work after the injury or |
|
|
|
|
|
of the home address. |
|
|
|
|
|
|
|
|
|
|
|
|
occupational disease. |
|
|
|
|
|
|
|
|
|
|
info. |
2 |
Department name: Enter the injured worker's |
11 State where hired: Enter the state where the injured |
|
|
|
department or area name where he/she normally |
|
|
|
|
|
|
worker was hired by the employer listed on this |
|
|
|
reports for work. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
application. |
|
|
|
|
|
|
|
|
|
|
|
|
|
injury/disease/death |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 Wage rate: Enter the injured worker's rate of pay, and |
12 Date employer notiied: Enter the date the employer |
|
|
|
then select how often it is received. (If the pay rate |
|
|
|
|
|
|
wasnotiiedoftheinjury,occupationaldiseaseordeath. |
|
|
|
being reported is not hourly, report the gross amount.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• If eight or more days of work will be missed, BWC |
13 State where supervised: Enter the state where the |
|
|
|
|
needs wage information for the 52 weeks prior to |
|
|
|
|
|
|
|
injuredworkerwassupervisedbytheemployerlisted |
|
|
|
|
the date of injury. Submit wage information using |
|
|
|
|
|
|
|
|
|
|
on this application. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
employer payroll reports, wage statement (BWC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
form C-94-A), W-2s, etc. |
|
|
|
|
|
|
|
|
|
14 Description of accident: Describe in detail the events |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 What days of the week do you usually work? What |
|
|
|
that caused the injury, occupational disease or death. |
|
|
|
are your regular work hours: Enter the days and |
|
|
|
Attach additional sheets, if necessary. |
|
|
and |
|
|
|
|
|
|
|
hours the injured worker normally works. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• If the days worked vary from week to week, list the |
15 |
|
Type of injury/disease and part of body affected: |
|
|
worker |
|
|
number of hours worked in an average week. |
|
|
|
|
|
|
Describethenatureoftheinjury,occupationaldisease |
|
|
5 |
Wages:Ifyoureceivedwagesduringdisability,please |
|
|
|
or death. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Indicate the part(s) of body injured, affected or that |
|
|
|
explain. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
caused the death. |
|
|
|
|
|
|
|
|
|
|
|
|
Injured |
6 Occupationorjobtitle:Entertheinjuredworker'stype |
|
|
|
Examples: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Laceration of irst toe, left foot; |
|
|
|
|
|
|
|
|
|
|
|
of occupation or actual job title at the time of injury, |
|
|
|
• Sprain of lower right back; etc. |
|
|
|
|
|
|
|
|
|
|
|
occupational disease or death. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16 Injured worker signature (injured workers only): |
|
|
|
7 |
Employer name: Enter the name of the injured |
|
|
|
|
|
|
Please |
read |
the |
Benefit application/medical |
|
|
|
|
worker's |
employer at the time of |
the |
injury, |
|
|
|
|
|
|
|
|
|
|
release information before signing and dating |
|
|
|
|
occupational disease or death. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
this form. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 Date of injury/disease: Enter the date injured worker |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
was injured. OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If the injured worker contracted an occupational |
|
|
|
|
|
|
|
|
|
|
|
|
Instructions |
|
|
|
|
|
disease, determine which of the following happened |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
continued |
|
|
|
|
|
most recently: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
on last page |
|
|
|
|
|
• The occupational disease was diagnosed by a medical provider; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[ |
|
|
|
|
• The irst medical treatment; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• The injured worker irst quit work, due to the occupational disease. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter this as the date of occupational disease. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|