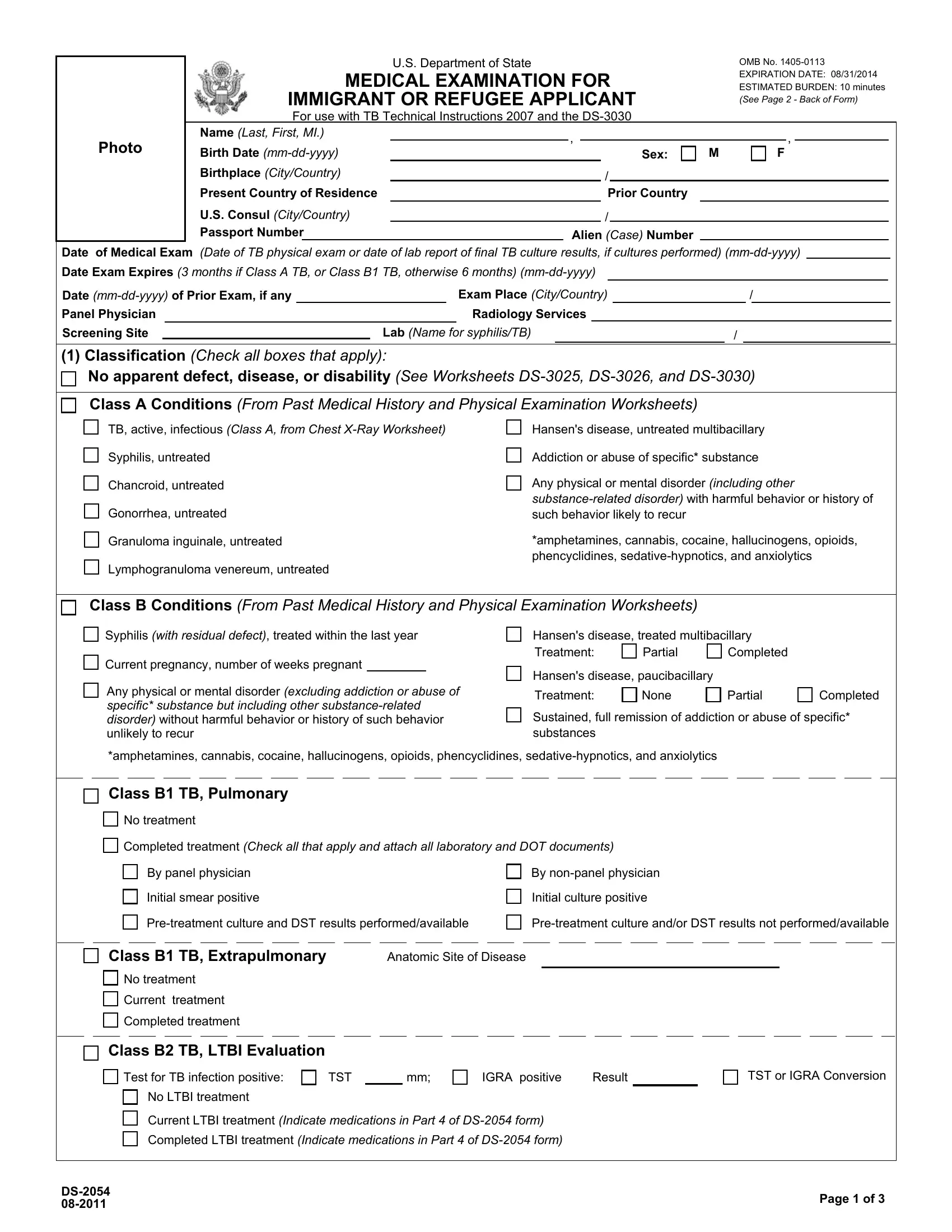
Embarking on the journey to becoming a lawful immigrant or refugee in the United States entails a thorough process, including the submission of the DS form, an integral document facilitated by the U.S. Department of State. It serves as a comprehensive medical examination form that must be completed by immigrant or refugee applicants, aligning with the TB Technical Instructions 2007 and the DS-3030. This document meticulously records personal information such as name, date of birth, and country of birth, alongside detailed medical examination results ranging from tuberculosis (TB) classifications to various infectious diseases assessments. Within its scope, the form categorizes medical conditions into Class A and Class B, distinguishing between more serious health conditions that could signify a public health risk and less severe issues. Additionally, the form addresses treatment histories, laboratory findings, and immunization records, ensuring that applicants meet the health standards required for entry into the U.S. It emphasizes the importance of transparency and accuracy, with the estimated burden of completing the form being around 10 minutes, although the impact on the applicant's journey is far more significant. By fulfilling the requirements outlined in the DS form, applicants take a crucial step toward their goal of residing in the United States, underpinning the process with a detail-oriented approach that underscores the intersection of public health and immigration policy.
| Question | Answer |
|---|---|
| Form Name | Form Ds 2054 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | ds2054 form ds 2054 |
Photo
|
|
U.S. Department of State |
|
|
|
|
|
|
|
OMB No. |
|||||
|
MEDICAL EXAMINATION FOR |
|
|
EXPIRATION DATE: 08/31/2014 |
|||||||||||
|
|
|
ESTIMATED BURDEN: 10 minutes |
||||||||||||
IMMIGRANT OR REFUGEE APPLICANT |
|
|
(See Page 2 - Back of Form) |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
For use with TB Technical Instructions 2007 and the |
|
|
|
|
|
|
|||||||||
Name (Last, First, MI.) |
|
, |
|
|
|
|
|
|
|
, |
|
|
|||
Birth Date |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Sex: |
|
M |
F |
||||||||
Birthplace (City/Country) |
|
|
|
/ |
|
|
|
|
|
|
|
|
|||
Present Country of Residence |
|
|
Prior Country |
|
|
|
|
|
|
||||||
U.S. Consul (City/Country) |
|
|
|
|
/ |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||||
Passport Number |
|
Alien (Case) Number |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Medical Exam (Date of TB physical exam or date of lab report of final TB culture results, if cultures performed)
Date |
|
|
|
Exam Place (City/Country) |
|
|
/ |
||||||
Panel Physician |
|
|
|
|
Radiology Services |
|
|
|
|
|
|||
Screening Site |
|
|
Lab (Name for syphilis/TB) |
|
/ |
|
|
|
|||||
|
|
||||||||||||
(1)Classification (Check all boxes that apply):
No apparent defect, disease, or disability (See Worksheets
Class A Conditions (From Past Medical History and Physical Examination Worksheets)
TB, active, infectious (Class A, from Chest
Syphilis, untreated
Chancroid, untreated
Gonorrhea, untreated
Granuloma inguinale, untreated
Lymphogranuloma venereum, untreated
Hansen's disease, untreated multibacillary
Addiction or abuse of specific* substance
Any physical or mental disorder (including other
*amphetamines, cannabis, cocaine, hallucinogens, opioids, phencyclidines,
Class B Conditions (From Past Medical History and Physical Examination Worksheets)
Syphilis (with residual defect), treated within the last year
Current pregnancy, number of weeks pregnant
Any physical or mental disorder (excluding addiction or abuse of specific* substance but including other
Hansen's disease, treated multibacillary |
|
||
Treatment: |
Partial |
Completed |
|
Hansen's disease, paucibacillary |
|
|
|
Treatment: |
None |
Partial |
Completed |
Sustained, full remission of addiction or abuse of specific* substances
*amphetamines, cannabis, cocaine, hallucinogens, opioids, phencyclidines,
Class B1 TB, Pulmonary
No treatment
Completed treatment (Check all that apply and attach all laboratory and DOT documents)
By panel physician
Initial smear positive
By
Initial culture positive
Class B1 TB, Extrapulmonary |
Anatomic Site of Disease |
No treatment |
|
Current treatment |
|
Completed treatment |
|
Class B2 TB, LTBI Evaluation
Test for TB infection positive: |
TST |
|
mm; |
IGRA positive |
Result |
No LTBI treatment |
|
|
|
|
|
Current LTBI treatment (Indicate medications in Part 4 of
Completed LTBI treatment (Indicate medications in Part 4 of
TST or IGRA Conversion
Page 1 of 3 |
||
|
Class B Tuberculosis - Continued
Class B3 TB, Contact Evaluation
TST |
|
mm |
IGRA negative |
IGRA positive IGRA Result |
No preventive treatment
Current preventive treatment (Indicate medications in Part 4 of
Completed preventive treatment (Indicate medications in Part 4 of
Alien Number
Relationship to Contact
Date Contact Ended
Type of Source Case TB (Mark only one and ATTACH DST RESULTS)
Pansusceptible TB
MDR TB (resistant to at least INH and rifampin)
Culture negative
Culture results not available
Class B Other (specify or give details on checked conditions from worksheets)
(2)Laboratory Findings (check all boxes that apply):
Syphilis:
Not done
|
|
|
|
Test Name |
|
Date(s) Run |
Negative |
Positive |
Titer 1 |
|
|
Notes |
||||||
|
Screening |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Confirmatory |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treated |
If treated, therapy: |
|
|
|
Date(s) treatment given |
|||||||||||||
|
|
Yes |
|
Benzathine penicillin, 2.4 MU IM |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
No |
|
Other (therapy, dose): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Test for
TST |
|
|
|
|
|
|
|
|
|
|
|
Date Applied |
|
|
|
|
Result (mm) |
||||||
IGRA |
|
|
|
|
|
|
|
|
|
|
|
Name of IGRA Test |
|
|
|
|
|
Date Drawn |
|
|
|||
Nil Value (IU/ml or number of cells) |
|
|
|
TB Response (TB- nil IU/ml or number of cells*) |
|
||||||
IGRA Interpretation: |
Positive |
Negative |
|
Indeterminate, Borderline, or Equivocal |
|||||||
*For
(3)Immunizations (See Vaccination Form, check all boxes that apply) Not required for refugee applicants.
Vaccine history complete
Incomplete vaccine history, no waiver requested
Vaccine history incomplete, requesting waiver (indicate type below)
Blanket waiver |
|
Individual waiver |
I certify that I understand the purpose of the medical examination and I authorize the required tests to be completed.
Applicant Signature |
Panel Physician Signature |
Date |
Page 2 of 3 |
(4) Tuberculosis Treatment Regimen
(Fill out if applicant has taken in the past, or is now taking TB medication. If drug doses or dates not known or not available, mark "unknown".)
Check if therapy currently prescribed (if current, don't mark "End Date")
Medication |
Dose/Interval |
|
Start Date |
|
End Date |
|||
|
|
|
|
(e.g., mg/day) |
|
|
||
|
|
Isonaizid (INH) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Rifampin |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
Pyrazinamide |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
Ethambutol |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Streptomycin |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
Other, specify |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Applicant's |
|
Date |
Remarks
PAPERWORK REDUCTION ACT AND CONFIDENTIALITY STATEMENTS
PAPERWORK REDUCTION ACT STATEMENT
Public reporting burden for this collection of information is estimated to average 10 minutes per response, including time required for searching existing data sources, gathering the necessary documentation, providing the information and/or documents required, and reviewing the final collection. You do not have to supply this information unless this collection displays a currently valid OMB control number. If you have comments on the accuracy of this burden estimate and/or recommendations for reducing it, please send them to: A/GIS/DIR, Room 2400
CONFIDENTIALITY STATEMENT
AUTHORITIES The information asked for on this form is requested pursuant to Section 212(a) and 221(d) and as required by Section 222 of the Immigration and Nationality Act. Section 222(f) provides that the records of the Department of States and of diplomatic and consular offices of the United States pertaining to the issuance and refusal of visas or permits to enter the United States shall be considered confidential and shall be used only for the formulation, amendment, administration, or enforcement of the immigration, nationality, and other laws of the United States. Certified copies of such records may be made available to a court provided the court certifies that the information contained in such records is needed in a case pending before the court.
PURPOSE The U.S. Department of State uses the facts you provide on this form primarily to determine your classification and eligibility for a U.S. immigrant visa. Individuals who fail to submit this form or who do not provide all the requested information may be denied a U.S. immigrant visa. Although furnishing this information is voluntary, failure to provide this information may delay or prevent the processing of your case.
ROUTINE USES If you are issued an immigrant visa and are subsequently admitted to the United States as an immigrant, the Department of Homeland Security will use the information on this form to issue you a Permanent Resident Card, and, if you so indicate, the Social Security Administration will use the information to issue a social security number. The information provided may also be released to federal agencies for law enforcement, counterterrorism and homeland security purposes; to Congress and courts within their sphere of jurisdiction; and to other federal agencies who may need the information to administer or enforce U.S. laws.
Page 3 of 3 |