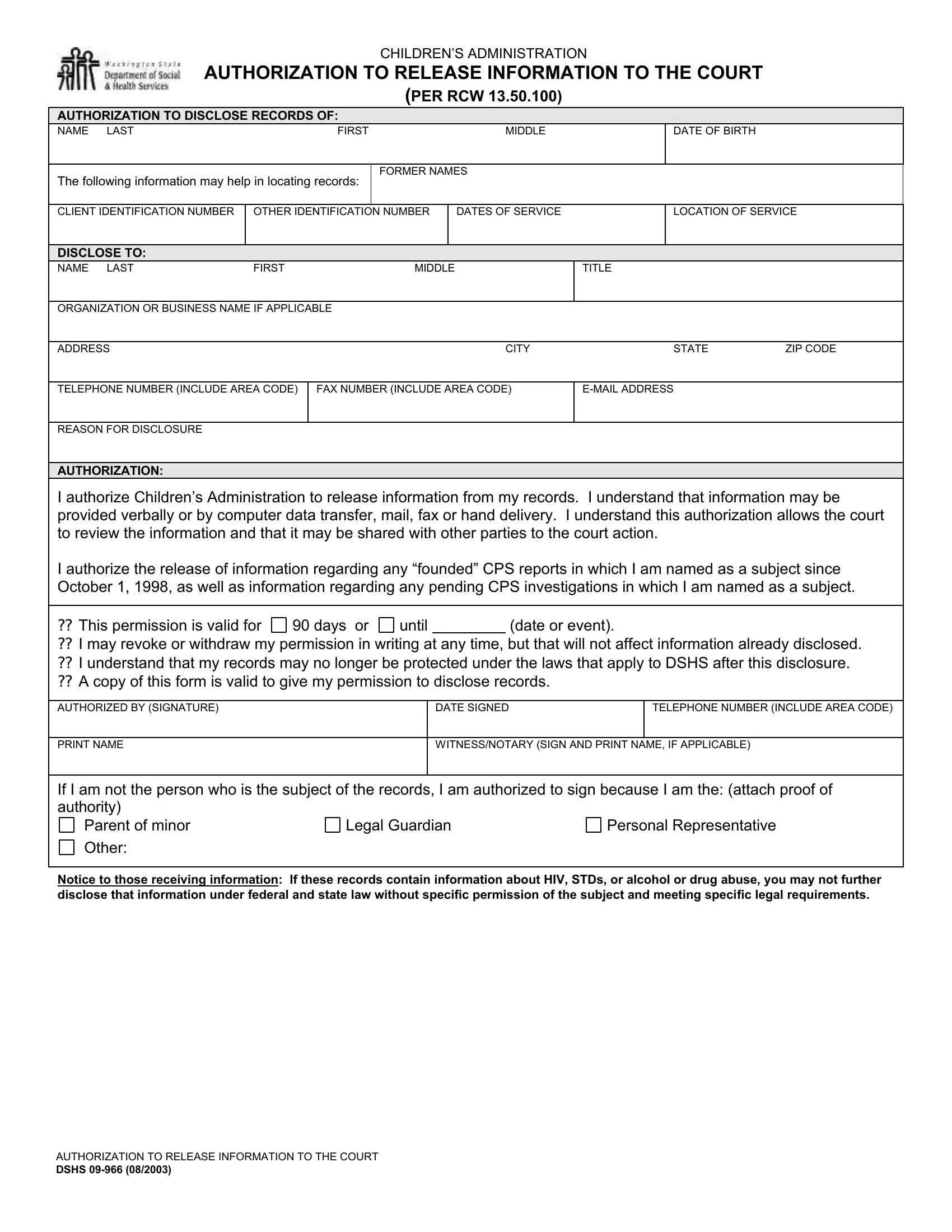
Engaging with the intricacies of legal documentation proves vital in navigating the complexities of the law, especially when it involves sensitive and protected information. The DSHS 09-966 form, a critical piece of documentation utilized by the Children's Administration, serves as a conduit for authorizing the release of information to the court, pursuant to RCW 13.50.100. This document encapsulates several crucial elements including the particulars of the individual whose records are sought (name, date of birth, former names, client identification, and service details) and the recipient of the information (name, title, organization, contact details). The form meticulously outlines the scope of information that can be disclosed, including records of any "founded" Child Protective Services (CPS) reports post-October 1, 1998, and pending investigations, thereby ensuring a balanced approach between the right to privacy and the administration of justice. Furthermore, it highlights the conditions under which this authorization operates, such as its validity period, the right of revocation, and the implications on the protection of the disclosed records. The necessity to include the authorization of the individual or a duly designated representative underscores the adherence to consent and legal authority in the handling of records. Designed to facilitate communication between welfare agencies and judicial bodies, the DSHS 09-966 form stands as a testament to the procedural safeguards and ethical considerations embedded in the pursuit of child welfare and justice.
| Question | Answer |
|---|---|
| Form Name | Dshs 09 966 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dshs information court, background check form dshs, dshs authorization pdf, dshs 966 information |
CHILDREN’S ADMINISTRATION
AUTHORIZATION TO RELEASE INFORMATION TO THE COURT
(PER RCW 13.50.100)
AUTHORIZATION TO DISCLOSE RECORDS OF:
NAME |
LAST |
|
FIRST |
MIDDLE |
|
DATE OF BIRTH |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
The following information may help in locating records: |
FORMER NAMES |
|
|
|
|
|||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
CLIENT IDENTIFICATION NUMBER |
OTHER IDENTIFICATION NUMBER |
|
DATES OF SERVICE |
|
LOCATION OF SERVICE |
|||||
|
|
|
|
|
|
|
|
|
|
|
DISCLOSE TO: |
|
|
|
|
|
|
|
|
|
|
NAME |
LAST |
FIRST |
|
MIDDLE |
|
TITLE |
|
|
||
|
|
|
|
|
|
|
||||
ORGANIZATION OR BUSINESS NAME IF APPLICABLE |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||
ADDRESS |
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
||
|
|
|
|
|
||||||
TELEPHONE NUMBER (INCLUDE AREA CODE) |
FAX NUMBER (INCLUDE AREA CODE) |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
REASON FOR DISCLOSURE |
|
|
|
|
|
|
|
|
|
|
AUTHORIZATION:
I authorize Children’s Administration to release information from my records. I understand that information may be provided verbally or by computer data transfer, mail, fax or hand delivery. I understand this authorization allows the court to review the information and that it may be shared with other parties to the court action.
I authorize the release of information regarding any “founded” CPS reports in which I am named as a subject since October 1, 1998, as well as information regarding any pending CPS investigations in which I am named as a subject.
?? This permission is valid for |
90 days or |
until |
(date or event). |
?? I may revoke or withdraw my permission in writing at any time, but that will not affect information already disclosed. ?? I understand that my records may no longer be protected under the laws that apply to DSHS after this disclosure. ?? A copy of this form is valid to give my permission to disclose records.
AUTHORIZED BY (SIGNATURE) |
DATE SIGNED |
TELEPHONE NUMBER (INCLUDE AREA CODE) |
|
|
|
PRINT NAME |
WITNESS/NOTARY (SIGN AND PRINT NAME, IF APPLICABLE) |
|
|
|
|
If I am not the person who is the subject of the records, I am authorized to sign because I am the: (attach proof of authority)
Parent of minor |
Legal Guardian |
Personal Representative |
Other: |
|
|
Notice to those receiving information: If these records contain information about HIV, STDs, or alcohol or drug abuse, you may not further disclose that information under federal and state law without specific permission of the subject and meeting specific legal requirements.
AUTHORIZATION TO RELEASE INFORMATION TO THE COURT
DSHS