In an environment where the conventional family structure faces diverse challenges, the role of non-related adults in the lives of needy children becomes increasingly vital. The DSHS 14-436 form, designed for Temporary Assistance for Needy Families (TANF)/State Family Assistance (SFA) for children living with unrelated adults, serves as a formal avenue to acknowledge and facilitate this unconventional yet essential support system. Individuals assuming the role of a parent, known as acting "in loco parentis," without court-ordered custody or guardianship, are required to fill out this document. It captures critical information ranging from agency details, particulars about the adult caregiver and the child's biological parents, to the specifics of the caregiver's relationship with the child. This comprehensive documentation process not only enables the adult to provide basic necessities, ensure educational attendance, and maintain the child's general welfare but also involves legal undertakings such as background checks to safeguard the child’s interests. The underlying principle of the form is to formalize the adult's commitment to act in the best interest of the child, embodying duties typically reserved for a parent, and to ensure the child's continuous access to benefits in a stable and secure environment.
| Question | Answer |
|---|---|
| Form Name | Dshs 14 436 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | printable loco parentis, CPS, Washington, TANF |
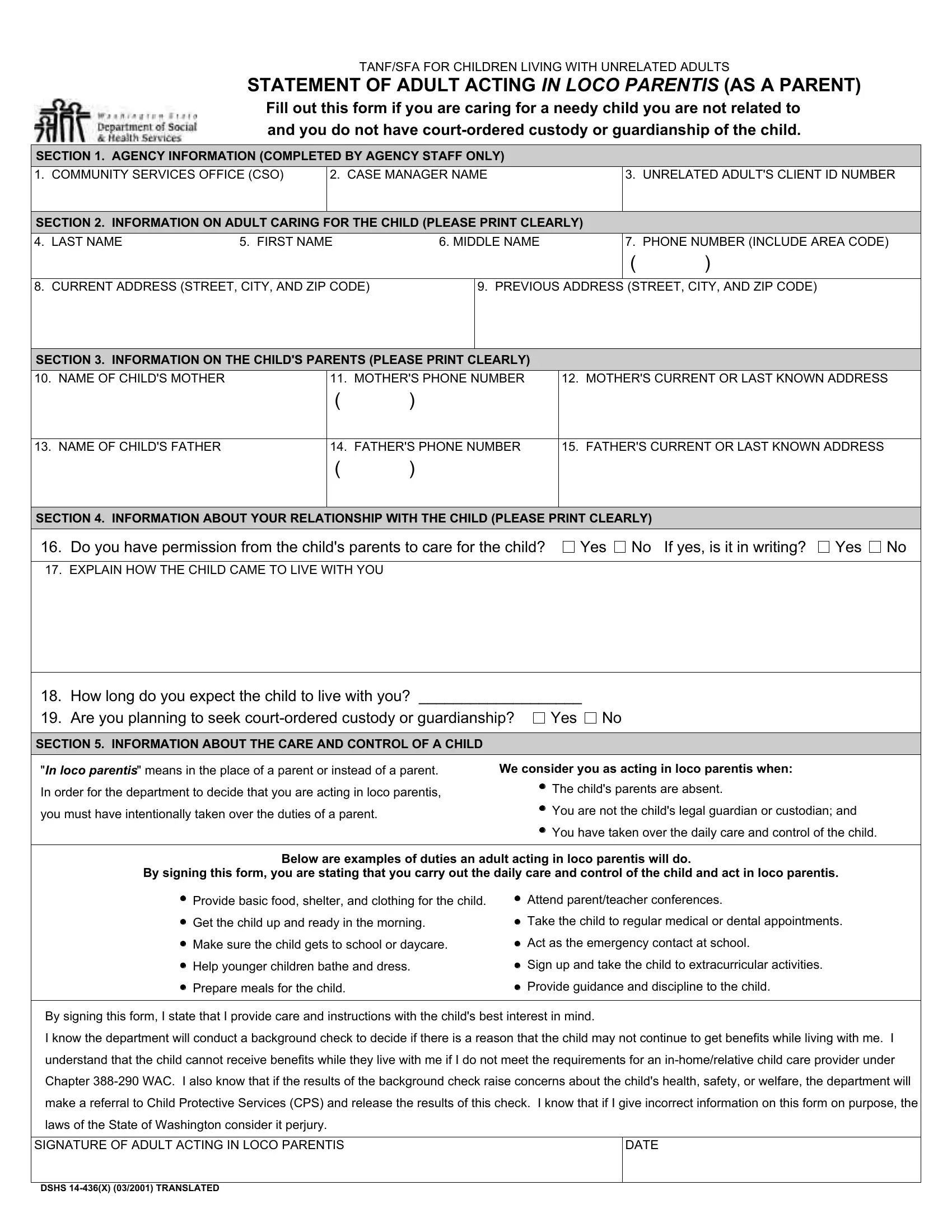
TANF/SFA FOR CHILDREN LIVING WITH UNRELATED ADULTS
STATEMENT OF ADULT ACTING IN LOCO PARENTIS (AS A PARENT)
Fill out this form if you are caring for a needy child you are not related to and you do not have
SECTION 1. AGENCY INFORMATION (COMPLETED BY AGENCY STAFF ONLY)
1. COMMUNITY SERVICES OFFICE (CSO)
2. CASE MANAGER NAME
3. UNRELATED ADULT'S CLIENT ID NUMBER
SECTION 2. INFORMATION ON ADULT CARING FOR THE CHILD (PLEASE PRINT CLEARLY)
4. LAST NAME |
5. FIRST NAME |
6. MIDDLE NAME |
7. PHONE NUMBER (INCLUDE AREA CODE)
()
8. CURRENT ADDRESS (STREET, CITY, AND ZIP CODE)
9. PREVIOUS ADDRESS (STREET, CITY, AND ZIP CODE)
SECTION 3. INFORMATION ON THE CHILD'S PARENTS (PLEASE PRINT CLEARLY)
10. NAME OF CHILD'S MOTHER |
11. MOTHER'S PHONE NUMBER |
12. MOTHER'S CURRENT OR LAST KNOWN ADDRESS |
()
13. NAME OF CHILD'S FATHER |
14. FATHER'S PHONE NUMBER |
15. FATHER'S CURRENT OR LAST KNOWN ADDRESS |
()
SECTION 4. INFORMATION ABOUT YOUR RELATIONSHIP WITH THE CHILD (PLEASE PRINT CLEARLY)
16. Do you have permission from the child's parents to care for the child? |
Yes No If yes, is it in writing? |
Yes No |
17. EXPLAIN HOW THE CHILD CAME TO LIVE WITH YOU
18. |
How long do you expect the child to live with you? ___________________ |
||
19. |
Are you planning to seek |
Yes No |
|
|
|
|
|
SECTION 5. INFORMATION ABOUT THE CARE AND CONTROL OF A CHILD |
|
|
|
"In loco parentis" means in the place of a parent or instead of a parent. |
We consider you as acting in loco parentis when: |
||
In order for the department to decide that you are acting in loco parentis, |
The child's parents are absent. |
|
|
you must have intentionally taken over the duties of a parent. |
You are not the child's legal guardian or custodian; and |
|
|
|
You have taken over the daily care and control of the child. |
Below are examples of duties an adult acting in loco parentis will do.
By signing this form, you are stating that you carry out the daily care and control of the child and act in loco parentis.
Provide basic food, shelter, and clothing for the child.
Get the child up and ready in the morning.
Make sure the child gets to school or daycare.
Help younger children bathe and dress.
Prepare meals for the child.
Attend parent/teacher conferences.
Take the child to regular medical or dental appointments.
Act as the emergency contact at school.
Sign up and take the child to extracurricular activities.
Provide guidance and discipline to the child.
By signing this form, I state that I provide care and instructions with the child's best interest in mind.
I know the department will conduct a background check to decide if there is a reason that the child may not continue to get benefits while living with me. I understand that the child cannot receive benefits while they live with me if I do not meet the requirements for an
SIGNATURE OF ADULT ACTING IN LOCO PARENTIS |
DATE |
|
|
DSHS