North Carolina Department of Health and Human Services
Application for Food and Nutrition Services
What are Food and Nutrition Services?
Food and Nutrition Services help households buy eligible food in authorized retail food stores. This will increase low-income household’s food buying power, so they can have more nutritious meals.
How Do I Apply for Food and Nutrition Services?
Step 1. Fill out this application: You have the right to receive an application upon request. If you cannot complete this application you will only need to provide a signature, legible name, and address. If you need assistance in completing this form, please let us know so that we can assist you.
Step 2. Turn in the application to your local agency as soon as possible: You can mail, fax
or bring the application to your local agency or apply online at https://epass.nc.gov/CitizenPortal/application.do. The date we get your application with your name, address, and signature on it, is also the start date of your Food and Nutrition Services application. If you are eligible for Food and Nutrition Services in the month you apply, the amount of Food and Nutrition Services you will get for that month depends on the date you turn in your application. The sooner you give us this application, the quicker you will know if you are able to get Food and Nutrition Services.
Step 3. Talk with us: A caseworker must interview you or someone you choose to represent you. This is to see if you can get Food and Nutrition Services. If you are unable to stay for your interview today, please tell the receptionist or a caseworker so that we can schedule an interview for you.
Information About Social Security Numbers, US Citizenship and Immigration Status
You can choose not to apply for yourself or members of your household and are not required to answer questions about Social Security Numbers (SSNs) and citizenship/immigration information for those you choose not to apply for. For each individual that you are applying for, you must provide information about SSNs and citizenship/immigration status. Providing a SSN is required by the Food and Nutrition Act for applicants seeking benefits. We will not share SSNs with US Citizenship and Immigration Service (USCIS). We will only use the SSNs you give us to do computer matches to check what you told us with State and Federal Agencies, Income and Eligibility Verification System (IEVS), other computer matching systems, program reviews and audits. This information may be verified through other sources when discrepancies are found and may affect your household’s eligibility and benefit level. You must be a United States (U.S.) citizen or an eligible alien and also meet other Food and Nutrition Services rules to get Food and Nutrition Services benefits. We will only contact USCIS to check the immigration status on the household members who give us their immigration documents. If an applicant does not provide this information, they will be ineligible for benefits. Household members must provide their financial information because it is needed to determine eligibility for individuals who are applying. Eligible household members who apply will be able to get benefits even though some people in the household are not applying for benefits. The amount of benefits will depend on the number of people requesting benefits.
Do You Need Assistance In Completing This Form?
If you need assistance in completing this application in order to apply for Food and Nutrition Services, please let us know so that we can assist you. Do you need assistance in completing this application? Yes No
Do You Need An Interpreter To Help You Apply For Food and Nutrition Services?
An interpreter can be provided, free of charge, if you need assistance in applying for Food and Nutrition Services. Would you like an interpreter to assist you? Yes No
Si usted necesita ayuda al solicitar los beneficios de Cupones de Alimentos, se le puede otorgar los servicios gratuitos de un intérprete, ¿Quisiera que un intérprete lo ayude? Sí No
Tell Us Do you need someone to apply for or use your Food and Nutrition Services?
If you want someone other than yourself to apply for, use, or obtain information about your benefits, please check yes below. If you check Yes, we will give or mail you a form. You and the person you want to help can complete the form and return it to our office. If you choose, this person will receive an EBT card and will have access to your Food and Nutrition Services. An Electronic Benefit Transfer Card (EBT) is a plastic card you use at the store to buy food. Do you need an Authorized Representative to help you get and/or use your Food and Nutrition Services? Yes No
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 1 of 10 |
When will I get my Food and Nutrition Services?
If you are able to get Food and Nutrition Services, you will get them within 30 calendar days from the date you turn in the application with your name, address, and signature. If you are applying for FNS and SSI at the same time from an institution the filing date is the date you are released from the institution. You may be able to get Food and Nutrition
Services within 7 calendar days if you qualify for expedited benefits. In order to evaluate you for expedited benefits make sure that you have provided us the needed information by answering the questions regarding your household’s income,
assets and expenses and if anyone is a migrant/seasonal farm worker. Your household may be in an emergency situation if:
•Your household's gross monthly income is less than $150 and your household's cash or money in the bank is $100 or less, or
•Your household's rent, mortgage and utilities are more than your household's gross monthly income and cash or money in the bank, or
•You or a member of your household is a migrant/seasonal farm worker.
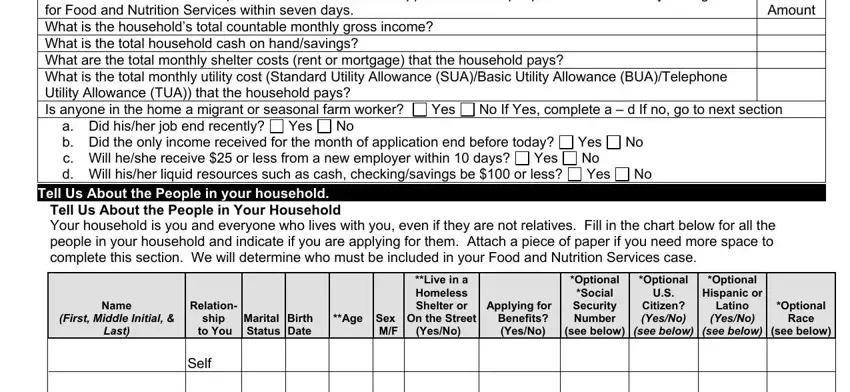
Expedited Benefits
The follow information will help us determine whether the applicant and the people in their home may be eligible |
|
for Food and Nutrition Services within seven days. |
|
|
Amount |
What is the household’s total countable monthly gross income? |
|
|
What is the total household cash on hand/savings? |
|
|
|
What are the total monthly shelter costs (rent or mortgage) that the household pays? |
|
What is the total monthly utility cost (Standard Utility Allowance (SUA)/Basic Utility Allowance (BUA)/Telephone |
|
Utility Allowance (TUA)) that the household pays? |
|
|
|
Is anyone in the home a migrant or seasonal farm worker? |
Yes |
No If Yes, complete a – d If no, go to next section |
a.Did his/her job end recently? Yes No
b.Did the only income received for the month of application end before today? Yes No
c.Will he/she receive $25 or less from a new employer within 10 days? Yes No
d.Will his/her liquid resources such as cash, checking/savings be $100 or less? Yes No
Tell Us About the People in your household.
Tell Us About the People in Your Household
Your household is you and everyone who lives with you, even if they are not relatives. Fill in the chart below for all the people in your household and indicate if you are applying for them. Attach a piece of paper if you need more space to complete this section. We will determine who must be included in your Food and Nutrition Services case.
Name
(FIRST, MIDDLE INITIAL, &
LAST)
|
|
|
|
|
**Live in a |
|
*Optional |
*Optional |
|
|
|
|
|
Homeless |
|
*Social |
U.S. |
Relation- |
|
|
|
|
Shelter or |
Applying for |
Security |
Citizen? |
ship |
Marital |
Birth |
**Age |
Sex |
On the Street |
Benefits? |
Number |
(YES/NO) |
to You |
Status |
Date |
|
M/F |
(Yes/No) |
(Yes/No) |
(see below) |
(SEE BELOW) |
|
|
|
|
|
|
|
|
|
*Optional |
|
Hispanic or |
|
Latino |
*Optional |
(YES/NO) |
Race |
(SEE BELOW) |
(see below) |
|
|
Self
*Social Security Numbers and Citizenship Information are not needed for those not applying for benefits.
*Eligibility or level of benefits are not affected if ethnicity or race is not answered. When the information is not provided the agency will collect the information by observation during the interview. Giving this information will help ensure program benefits are distributed without regard to race, color or national origin (this information is used for statistical purposes only).
*RACE: Choose one or more numbers that apply and enter above for Race:
1 - American Indian/Alaskan Native, 2 – Asian, 3 – Black/African American, 4 – Native Hawaiian/Other Pacific Islander and 5 – White
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 2 of 10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
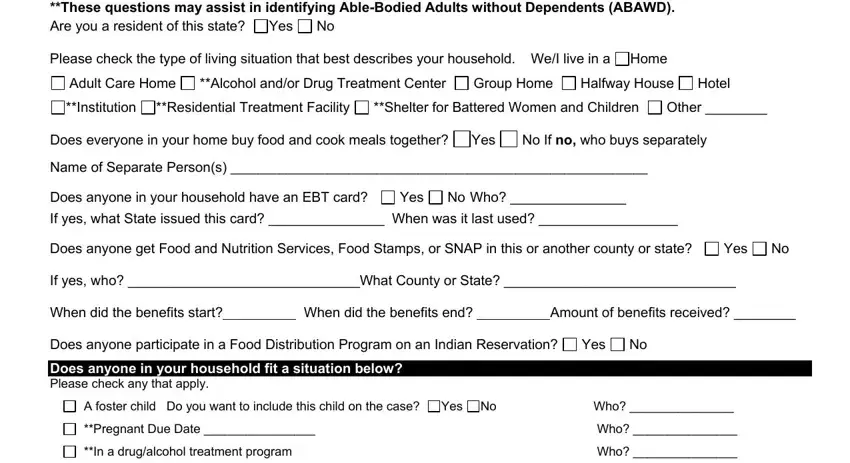
**These questions may assist in identifying Able-Bodied Adults without Dependents (ABAWD). |
|
|
Are you a resident of this state? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
Please check the type of living situation that best describes your household. |
We/I live in a |
Home |
|
|
Adult Care Home |
**Alcohol and/or Drug Treatment Center |
Group Home |
Halfway House |
Hotel |
|
**Institution |
**Residential Treatment Facility |
**Shelter for Battered Women and Children |
Other ________ |
|
Does everyone in your home buy food and cook meals together? |
Yes |
No If no, who buys separately |
|
Name of Separate Person(s) ____________________________________________________________ |
|
|
|
Does anyone in your household have an EBT card? |
Yes |
No Who? _______________ |
|
|
|
|
If yes, what State issued this card? _______________ When was it last used? __________________ |
|
|
Does anyone get Food and Nutrition Services, Food Stamps, or SNAP in this or another county or state? |
Yes |
No |
If yes, who? ______________________________What County or State? ______________________________ |
|
When did the benefits start? |
|
|
When did the benefits end? |
|
Amount of benefits received? ________ |
|
|
|
|
|
|
|
|
|
|
Does anyone participate in a Food Distribution Program on an Indian Reservation? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Does anyone in your household fit a situation below? |
|
|
|
|
|
|
|
|
|
|
Please check any that apply. |
|
|
|
|
|
|
|
|
|
|
|
|
|
A foster child |
Do you want to include this child on the case? |
Yes |
|
No |
|
|
Who? _______________ |
|
**Pregnant Due Date ________________ |
|
|
|
|
|
|
Who? _______________ |
|
**In a drug/alcohol treatment program |
|
|
|
|
|
|
|
Who? _______________ |
|
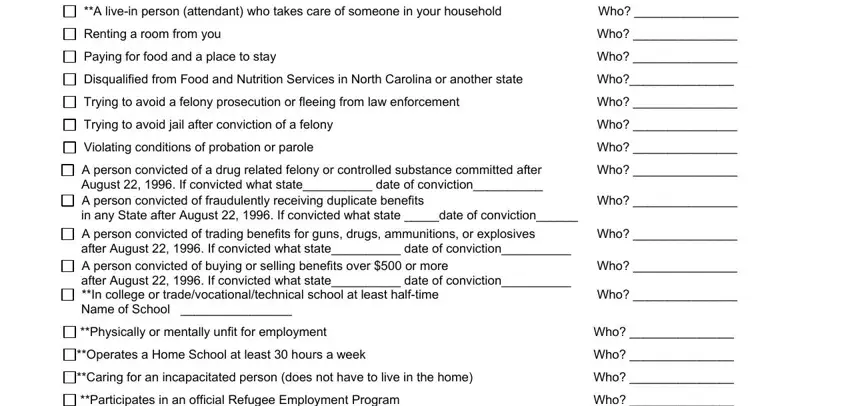
**A live-in person (attendant) who takes care of someone in your household |
|
|
Who? _______________ |
|
Renting a room from you |
|
|
|
|
|
|
|
|
Who? _______________ |
|
Paying for food and a place to stay |
|
|
|
|
|
|
|
Who? _______________ |
|
Disqualified from Food and Nutrition Services in North Carolina or another state |
Who?_______________ |
|
Trying to avoid a felony prosecution or fleeing from law enforcement |
|
|
|
|
Who? _______________ |
|
Trying to avoid jail after conviction of a felony |
|
|
|
|
|
|
Who? _______________ |
|
Violating conditions of probation or parole |
|
|
|
|
|
|
Who? _______________ |
|
A person convicted of a drug related felony or controlled substance committed after |
Who? _______________ |
|
August 22, 1996. If convicted what state__________ date of conviction__________ |
|
|
|
|
|
A person convicted of fraudulently receiving duplicate benefits |
|
|
|
|
|
Who? _______________ |
|
in any State after August 22, 1996. If convicted what state _____date of conviction______ |
|
|
|
|
|
A person convicted of trading benefits for guns, drugs, ammunitions, or explosives |
Who? _______________ |
|
after August 22, 1996. If convicted what state__________ date of conviction__________ |
|
|
|
|
|
A person convicted of buying or selling benefits over $500 or more |
|
|
|
|
Who? _______________ |
|
after August 22, 1996. If convicted what state__________ date of conviction__________ |
|
|
|
|
|
**In college or trade/vocational/technical school at least half-time |
|
|
|
|
|
Who? _______________ |
|
Name of School |
________________ |
|
|
|
|
|
|
|
|
|
|
|
|
**Physically or mentally unfit for employment |
|
|
|
|
|
|
Who? _______________ |
|
**Operates a Home School at least 30 hours a week |
|
|
|
|
|
|
Who? _______________ |
|
**Caring for an incapacitated person (does not have to live in the home) |
|
|
Who? _______________ |
|
**Participates in an official Refugee Employment Program |
|
|
|
|
|
Who? _______________ |
|
**Unable to work due to alcohol and/or drug addiction |
|
|
|
|
|
Who? _______________ |
|
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 3 of 10 |
**These questions may assist in identifying Able-Bodied Adults without Dependents (ABAWD).
What assets do people in your household have?
Assets are valuable items that you own such as cash or bank accounts. We will determine if verification is needed and if it is accessible to you.
Has anyone in your household transferred assets in the last 3 months in order to receive Food and Nutrition Services? Yes No
Does your household own any of the assets listed below?
Please check all the assets you own, someone else in your household owns, or jointly own with non-household member.
|
|
Value or |
Business Name and |
Type of Asset |
Who Does This Belong To? |
Worth |
Account Number |
Cash |
|
|
|
Checking and/or Savings Acct |
|
|
|
Retirement Accounts |
|
|
|
Mutual Funds or Trust Funds |
|
|
|
Prepaid Burial Contracts |
|
|
|
Certificates of Deposit (CD’s) |
|
|
|
Stocks or Bonds |
|
|
|
Other Assets Not Listed |
|
|
|
What money do people in your household get from work?
**Does anyone in your household work?
Please provide verification for the previous month. Example: If it is now the month of June, we will need verification of ALL income received in the month of May. Don’t delay turning in your application if you don’t have the verification
because you can turn it in later. Include Full-Time, Part-Time, Day Work, Temporary Work, Work Study for College, and Tips.
Employer (Name, Address, Phone Number if Available)
Gross Pay (Pay Before Taxes)
How Often |
Last date |
Day of |
Hours |
is Pay |
Pay |
Week Pay |
Per |
Received? |
Received |
Received |
Week |
|
|
|
|
**Is anyone in your household self-employed? |
Yes |
No If yes, complete below. |
Please provide verification of the previous year’s tax records. If tax records are not available provide verification of |
income and receipts for business expenses for the past 12 months. Don’t delay turning in your application if you don’t
have the verification because you can turn it in later.
Examples are babysitting, selling Avon or other products, farming, doing hair, renting houses, doing yard work for other people or odd jobs.
|
|
Hours Per |
Business Name |
Type of Business |
Week |
|
|
|
Gross Monthly |
Monthly |
Income |
Expenses |
|
|
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 4 of 10 |
**These questions may assist in identifying Able-Bodied Adults without Dependents (ABAWD).
Is anyone getting ready to start a new job?
No If yes, complete below.
Employer
(Name, Address, Phone Number If Available)
Gross
Pay (Pay Before Taxes)
How Often is Pay Received?
Date of
First Pay
Received
Day of the
Week Pay
Received
Hours Days
Per Worked Week Per Week
**Has anyone stopped working in the past 30 days?
No If yes, please complete below.
Employer
(Name, Address, Phone Number if Available)
|
Date Last Pay |
Gross |
|
Received or Will |
Amount of |
End Date |
Be Received |
Last Pay |
|
|
|
Total Hours
Worked in
Past 30
Days
Is anyone a migrant or seasonal farm worker? |
Yes |
No If yes, who? ______________________________ |
Date started working? ___________________________________________________________________________
Place working & phone number? ____________________________________________________________
Is anyone on strike? |
Yes |
No If yes, who? _____________________________________________ |
Last date worked? _______________Place worked & phone number? ______________________________
Tell us about any volunteer work or participation in a work training program.
*Does anyone work as a volunteer or participate in a work training program?
|
Name of Volunteer Site |
|
|
|
Hours |
|
or Work Training |
Site Address and Phone Number (if |
Start |
End |
Per |
Name |
Program |
Available) |
Date |
Date |
Week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What money does your household get from other sources?
We need to know the money or checks you get other than from work. Please check off all of the following that applies to your household:
Adoption, Foster Care, or Guardianship Payments Annuities, Pensions, or Retirement
Alimony
Child Support from parent or Child Support from the Court Educational Scholarships**
Military Allotment
Money from friends or relatives that is not a loan and you don’t have to pay back
Payments for the sale of an asset (such as a car, boat, mobile home or house)
Private Disability**
DSS-8207 (Rev. 12-2018)
Economic and Family Services
Social Security**
Special Assistance (SA)** Supplemental Security Income (SSI)** Unemployment Benefits** Veterans Benefits**
Work First/TANF** Interest and Dividends Workers Compensation** Other ________________
My Household does not get any other money
Page 5 of 10
**These questions may assist in identifying Able-Bodied Adults without Dependents (ABAWD).
For all items checked above, complete below:
|
Type of |
|
|
Who Gets the |
|
|
Who Gives the |
|
|
Phone Number and Address of |
|
|
|
|
|
How |
|
|
|
|
|
|
|
|
|
|
|
Person/Organization That Gives You |
|
|
How |
|
|
|
|
Date Last |
|
|
Money |
|
|
Money? |
|
|
Money? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Money |
|
|
Much? |
|
|
Often? |
|
|
Received |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is any of the income listed above child support? Yes |
No If yes, is the child support court ordered? |
Yes |
No |
If yes, what is the Court Order Number ___________ Date Established ___________ Obligated Amount ________?
Please tell us about your household bills.
Please complete this section for all expenses your household is responsible for paying.
|
Name, Address, Phone Number to |
Amount |
How |
Who Pays the |
Expense Type |
Whom You Pay the Bill |
Billed |
Often |
Bill? |
|
|
|
Paid? |
|
Rent or Mortgage |
|
|
|
|
Lot Rent |
|
|
|
|
Property Taxes (If not |
|
|
|
|
included in mortgage) |
|
|
|
|
Homeowners Insurance (If |
|
|
|
|
not included in mortgage) |
|
|
|
|
Homeowners Dues (HOA)
Check the boxes next to the utility cost your household is responsible for paying that is paid separate from your rent.
Electricity |
LP/Natural Gas |
Utility Excess (Public Housing) |
Water/Sewage |
Telephone/Cell Phone Name of phone company _____________________
How do you heat your home? _____________________ How do you cool your home? ___________________
Were you a member of a household that received a Low Income Energy Assistance Program (LIEAP) check at your current address within the past 12 months? Yes No
Do you receive Section 8 or HUD Assistance?
Help Paying Bills
Does any agency, organization, or person (including Section 8) outside your household help pay any of your rent or utilities? Yes No If yes, complete questions below.
|
Name, Address, Phone Number of the |
Was the |
|
|
How |
Date of |
Which Bill is Paid? |
Person That Pays the Bill? |
Money Given |
Amount |
Often |
Last |
|
|
to You? |
|
Paid |
Paid? |
Payment |
|
|
Yes |
No |
|
|
|
|
|
Yes |
No |
|
|
|
|
|
Yes |
No |
|
|
|
|
|
Yes |
No |
|
|
|
DSS-8207 (Rev. 12-2018)
Economic and Family Services
Page 6 of 10
Please tell us about your other bills.
Do you or anyone in your household pay for child or disabled adult care? Child/disabled adult care transportation expenses $
Yes No If yes, complete questions below.
|
|
|
|
|
|
|
|
Number |
Who Gets |
Who Pays |
Name, Address, Phone |
How |
How |
Start |
Why is |
Date of |
of |
the Care? |
for the |
Number of Care Provider or |
Much |
Often |
Date |
Care |
Last |
Hours |
|
Care? |
Babysitter |
is |
Paid? |
|
Needed? |
Payment |
Per |
|
|
|
Paid? |
|
|
|
|
Week |
Does any agency, organization or person outside your household help pay any of your childcare? complete questions below.
Name, Address, Phone Number of the Person That Pays the Bill
Court Ordered Child Support
Does your household pay court ordered child support for children outside your home? Include court ordered health insurance payments. Yes No If yes, complete questions below.
Who Pays the |
Name of |
Child Support? |
Child? |
|
|
Name, Address and Phone Number of |
Amount |
Start |
Person That Pays the Child Support |
Paid |
Date |
|
|
|
Medical Bills for Disabled or Age 60 or Over
(A disabled person usually gets disability payments from a government agency such as Social Security, SSI, Veterans Benefits for 100% Disability, or Medicaid for disabled persons.)
Is anyone age 60 or over or disabled? |
Yes |
No If yes, who? ______________________. When did the disability |
begin? ______________________ Who made the disability determination? _________________________________
If yes, we need to know the medical bills you have or are responsible for paying. Medical bills include, but are not limited to:
•Health and hospital insurance premiums or co- payments
•Food and/or veterinary care for a trained service animal
•Transportation and lodging to get medical treatment
•Medicare Premiums
•Doctor and hospital bills
•Prescription and over-the-counter medications and medical supplies such as aspirin, diabetic supplies and eye glasses
•Rental and purchase of medical equipment and supplies
•Prescribed eye glasses and contact lenses
•Dentures, hearing aids, and prostheses
•Payments for aides, attendants, and nurses
When Did the |
Name, Address, Phone Number of |
Expense Start? |
Medical Provider |
|
|
Does any agency, organization or person outside your household help pay any of your medical bills? complete below.
Who Pays the Bill? _______________ Which Bill Is Paid? _______________ Amount per month _______________
Who Pays the Bill? _______________ Which Bill Is Paid? _______________ Amount per month _______________
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 7 of 10 |
By signing this application, I am stating that:
1.I have told the truth on this form and I did not lie or hide information to get benefits that my household should not get.
2.I understand the Food and Nutrition Services rules and what I must do to get Food and Nutrition Services.
3.I agree to provide information about what I have said so that my application can be processed. I am aware the information I give may be disclosed to other Federal and State agencies for official examination and to law enforcement officials for the purpose of apprehending persons fleeing to avoid the law.
4.I give permission to the local agency to get proof of what I have said from any person, business or other outside agencies, but not limited to: employers, banks, savings and loans, landlords, etc.
5.Under penalty of perjury, I have told the truth about information on the application, including the information concerning citizenship and alien status for all the members applying for benefits/assistance.
6.I understand my expenses may be used to figure my Food and Nutrition Services amount. If I do not tell you about some of my expenses and/or verify them, they may not be used in the budget to calculate the amount of my benefits.
7.I have read, understand, and received the Program Information and Rights and Responsibilities form.
8.I have the right to ask for a hearing if I think my case is wrong. I have 90 calendar days to ask for a hearing. Unless you ask for a hearing by then, you cannot have one. A household member or someone else such as a lawyer, friend, or relative can represent
me at a fair hearing.
9. I am aware of the Intentional Program Violation Penalties.
Individuals found to have committed an Intentional Program Violation either through an administrative disqualification hearing or by a Federal, State or local court, shall be ineligible to participate in the Food and Nutrition Services:
For A Period of Twelve months for the first Intentional Program Violation, Twenty-four months for the second violation and Permanently for the third violation of any Intentional Program Violation. Additional Program Violations:
•If you use your food assistance benefits to buy nonfood items, such as alcohol or cigarettes, or to pay on credit accounts you will lose your benefits.
•Giving wrong information knowingly may also mean we may reduce your benefits, you may have to repay benefits, may be subject to criminal prosecution or not able to get benefits for twenty-four months.
•If a court finds you guilty of trading Food and Nutrition Services for controlled substances, you will lose Food and Nutrition Services for two years for the first violation and permanently for the second violation.
•If a court finds you guilty of buying, selling, or trading benefits $500 more, trading benefits for firearms, drug trafficking, ammunition, or explosives after August 22, 1996 you may lose Food and Nutrition Services forever.
•You will not get Food and Nutrition Services for 10 years if you are found guilty of getting or trying to get Food and Nutrition Services in more than one household at a time. This penalty happens if you give wrong information about who you are or where you live.
•If you intentionally break any of the rules above you may not be able to get Food and Nutrition Services permanently, and may be fined up to $250,000 and/or jailed up to 20 years. You may also be ineligible for Food and Nutrition Services for an additional 18 months, if court ordered.
•I understand the information I provided on the application will be subject to verification by Federal, State or local officials to determine if the information is factual; that if any information is incorrect, Food and Nutrition Services may
be denied and I may be subject to criminal prosecution for knowingly providing incorrect information. Voter Registration
If you are not registered to vote where you live now, would you like to apply to register to vote here today? Yes No
IF YOU DO NOT CHECK EITHER BOX, YOU WILL BE CONSIDERED TO HAVE DECIDED NOT TO REGISTER TO VOTE AT THIS TIME. Applying to register or declining to register to vote will not affect the amount of assistance that you will be provided by this agency. If you would like help in filling out the voter registration application form, we will help you. The decision whether to seek or accept help is yours. You may fill out the application form in private. If you believe that someone has interfered with your right to register or to decline to register to vote, your right to privacy in deciding whether to register or in applying to register to vote or your right to choose your own political party or other political preference, you may file a complaint with the North Carolina Bipartisan State Board of Elections and Ethics Enforcement. If you require assistance with voter registration, you can call the North Carolina Bipartisan State Board of Elections and Ethics Enforcement at 1-866-522-4723.
Your Signature or Authorized Representative |
|
|
|
|
Date Signed |
|
|
Witness Signature (if signature is an X) |
|
|
|
Date Signed |
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
|
Middle Initial |
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residence Address |
|
|
|
|
City |
State |
|
Zip Code |
|
(If different from residence address) |
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
City |
State |
|
Zip Code |
|
Home Phone |
Cell Phone |
Message Number |
|
Telephone Company Provider |
|
Language you speak |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**AGENCY USE ONLY** |
|
|
|
|
|
Required Caseworker Signature |
|
|
|
Date of Interview |
Telephone Office visit |
|
For information regarding the Teen Pregnancy Prevention Initiative contact your local Health Department or call the DHHS Customer Service Center at 1- 800-662-7030. For information regarding services provided for Healthy Marriages contact your local agency.
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 8 of 10 |
Program Information
Rights and Responsibilities
Changes You Must Report and How to Report Them
Your caseworker will give you a Change Report Form for your household’s situation and explain it to you.
This form will tell you all the changes you must report to us and when to report them.
When you have a change, fill out the form and mail it to us. You may also call your caseworker or come in to our office to report changes. Your caseworker will contact you about the change.
Information About Social Security Numbers
You must provide the Social Security Number (SSN) used by each person in your household that you apply for. If you need help getting a SSN, ask your caseworker for help. We will only give Food and Nutrition Services to the eligible people who give us
their SSN. Eligible household members who apply will be able to get benefits even though some people in the household are not applying for benefits. We will use the SSN’s you give us to do computer matches and check what you told us with State and Federal
Agencies.
Information About U.S. Citizenship and Immigration Status
You must be a United States (U.S.) citizen or an eligible alien to get Food and Nutrition Services. You must also meet other Food and Nutrition Services rules.
You must provide the US Citizenship and Immigration Service (USCIS) documents used by each person in your household that you apply for. We will only give Food and Nutrition Services to the eligible people who give us their legal USCIS documents. Eligible household members who apply will be able to get benefits even though some people in the household are not applying for benefits.
We will only contact USCIS to check the immigration status of the people who give us their immigration documents.
Food and Nutrition Services Rules
The following rules apply for getting and using Food and Nutrition Services:
Don't hide, lie or give wrong information on purpose to get Food and Nutrition Services benefits.
Don't use Food and Nutrition Services to buy non-food items like alcohol or tobacco.
Don't trade or sell your Food and Nutrition Services.
Don't use someone else's Food and Nutrition Services for yourself.
Don't use your Food and Nutrition Services for someone else.
Don't use your Food and Nutrition Services to pay on any kind of credit account even if it is for eligible Food and
Nutrition Services items or pay for food purchased on credit with Food and Nutrition Services benefits.
DO cooperate with state and federal personnel in a Quality Control review.
Penalties for Breaking the Rules of the Food and Nutrition Services Program
If you intentionally break any of the rules above, you may not be able to get any more Food and Nutrition Services from one year to permanently and may be fined up to $250,000 and/or jailed up to twenty years or both. You may also be subject to prosecution under applicable Federal and State laws. You may also be barred from the Food and Nutrition Services an additional 18 months if court ordered.
Giving wrong information may also mean we will reduce your benefits, or you may be required to repay benefits.
If a court finds you guilty of buying, selling, or trading $500 or more after August 22, 1996 in Food and Nutrition Services, you may lose Food and Nutrition Services permanently.
If a court finds you guilty of trading Food and Nutrition Services for firearms, ammunition, or explosives after August 22, 1996 you will lose Food and Nutrition Services permanently.
If a court finds you guilty of trading Food and Nutrition Services for controlled substances, you will lose Food and Nutrition Services for two years the first time and permanently.
You will not get Food and Nutrition Services for 10 years if you are found guilty of getting or trying to get Food and Nutrition Services in more than one household at a time. This penalty happens if you give wrong information about who you are or where you live.
Information About Hearings
You have the right to ask for a hearing in person, by telephone or in writing, if you think your case is wrong. You have 90 calendar days to ask for a hearing. Unless you ask for a hearing by then, you cannot have one. A household member or someone else such as a lawyer, friend, or relative can represent you at a fair hearing. Free legal advice may be available. Contact Legal Aid of North Carolina office at 1-866-219-5262, Street: 224 South Dawson St. Raleigh, NC 27601, Mailing: PO Box 26087 Raleigh, NC 27611.
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 9 of 10 |
Information About Work and Training Rules
Some people have to work or attend training to get Food and Nutrition Services. If this is true for you or for other people in your household, we will tell you. You will have to follow the rules about work and training to get Food and Nutrition Services.
We Check What You Tell Us
I understand the information I provided on the application will be subject to verification by Federal, State or local officials to determine if the information is factual and that if any information is incorrect Food and Nutrition Services may be denied and I may be subject to criminal prosecution for knowingly providing incorrect information.
All eligibility procedures are strictly supported by the Food and Nutrition Services policies. Other program’s time limits or requirements do not affect your Food and Nutrition Services benefits. Your household may not be denied food assistance because your household has been denied benefits from other programs.
I am aware of the information I give may be disclosed to other Federal and State agencies for official examination, and to law enforcement officials for the purpose of apprehending persons fleeing to avoid the law.
If you have a Food and Nutrition Services claim against you, we will give your answers and Social Security Numbers to federal and state agencies, as well as private claims collection agencies, to collect the overpayment.
We Must Obtain Data
We are required to request racial and ethnic data on participating households. The information is voluntary; neither your eligibility nor Food and Nutrition Services benefits will be affected if you choose not to provide it. Giving this information will help ensure program benefits are distributed without regard to race, color or national origin (this information is used for statistical purposes only).
You Will Not Be Discriminated Against
In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, sex, religious creed, disability, age, political beliefs, or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA.
Persons with disabilities who require alternative means of communication for program information (e.g. Braille, large print, audiotape, American Sign Language, etc.), should contact the Agency (State or local) where they applied for benefits. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800) 877-8339. Additionally, program information may be made available in languages other than English.
To file a program complaint of discrimination, complete the USDA Program Discrimination Complaint Form, (AD-3027) found online at: http://www.ascr.usda.gov/complaint_filing_cust.html, and at any USDA office, or write a letter addressed to USDA and provide in the letter, all of the information requested in the form. To request a copy of the complaint form, call (866) 632-9992. Submit your completed form or letter to USDA by:
Mail: U.S. Department of Agriculture
Office of the Assistant Secretary for Civil Rights
1400 Independence Avenue, SW
Washington, D.C. 20250-9410
Fax: (202) 690-7442; or
Email: program.intake@usda.gov.
This institution is an equal opportunity provider.
Getting Help With Your Telephone Bill
If you receive Supplemental Security Income (SSI), Food and Nutrition Services, Medicaid, Federal Public Housing (Sec. 8 Housing Assistance), or Veterans Pension and Survivors Benefit you may be eligible for a local telephone service discount.
Lifeline provides recipients a discount on monthly telephone service purchased from participating providers. Recipients can also purchase discounted broadband from participating providers. Discounts will apply to stand-alone broadband, bundled voice- broadband packages, either fixed or mobile and stand-alone voice service.
The Link-Up Program allows recipients who are Native Americans residing on federally recognized tribal lands a discount toward the cost of connecting local telephone service.
Households interested in these services must contact their telephone company to apply.
DSS-8207 (Rev. 12-2018) |
|
Economic and Family Services |
Page 10 of 10 |