
If you need to fill out form dss ea 284, you don't need to install any kind of programs - just try using our online tool. To make our tool better and less complicated to use, we continuously develop new features, considering suggestions from our users. This is what you would need to do to get started:
Step 1: Click on the "Get Form" button above on this page to get into our editor.
Step 2: This tool offers you the opportunity to change most PDF forms in various ways. Improve it by adding customized text, adjust existing content, and put in a signature - all within a few clicks!
It is actually simple to fill out the form adhering to this practical guide! Here is what you should do:
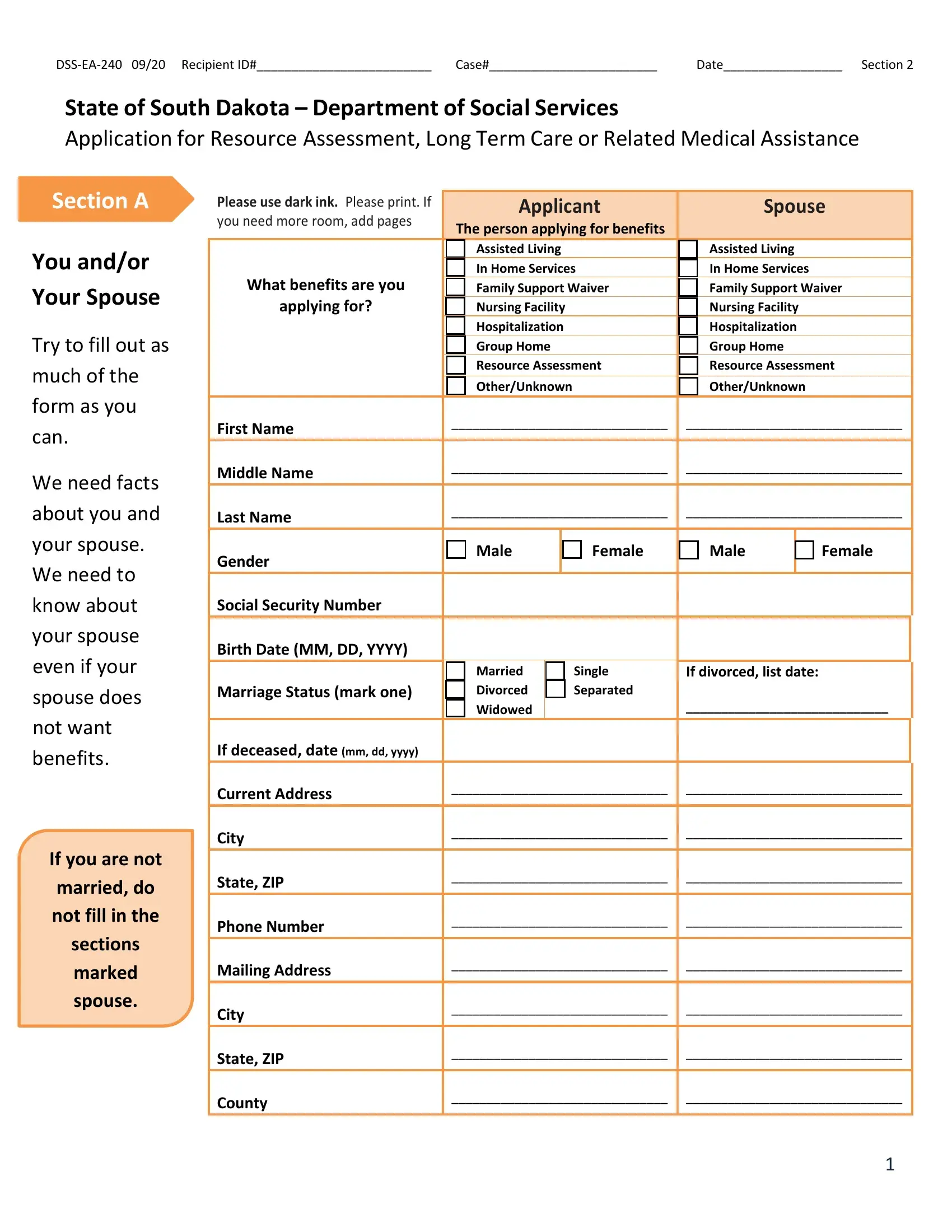
1. Whenever completing the form dss ea 284, ensure to complete all essential blanks within the corresponding form section. It will help facilitate the process, enabling your details to be processed fast and properly.
2. After filling in the last step, go on to the next step and complete all required details in these blanks - We need facts about you and your, If you are not married do not fill, sections marked spouse, Current Address, City, State ZIP, Phone Number, Mailing Address, City, State ZIP, and County.
You can certainly get it wrong when filling out the County, therefore you'll want to go through it again before you'll send it in.
3. The next step is generally fairly uncomplicated, Section A, Section A, Applicant, Spouse, You andor Your Spouse continued, Email, Live in South Dakota, Plan to stay in South Dakota, Hispanic or Latino optional, Yes, Yes, Yes, Yes, Yes, and Yes - every one of these empty fields has to be filled in here.
4. Filling in Citizenship, Provide citizenship, documentation, if not a US, citizen, Are you a US Citizen If yes go to, Are you a refugee or legally, mmddyyyy, Are you registered with the US, Yes, Yes, If no give facts below, If no give facts below, Yes, and Yes is essential in the next section - make sure you devote some time and be mindful with each and every field!
5. To finish your form, the final part includes a couple of extra blank fields. Filling in Section C, People Helping You, Person helping with legal matters, Power of Attorney, Guardian, Yes, Name, Address, City State Zip Code, Phone, Email, Person helping you fill out this, Yes, Name, and Relationship or Organization should finalize everything and you can be done in no time!
Step 3: Prior to moving forward, double-check that form fields were filled in as intended. As soon as you think it is all good, click on “Done." Find your form dss ea 284 as soon as you sign up for a free trial. Readily get access to the pdf file inside your personal account page, together with any edits and adjustments automatically saved! FormsPal ensures your data confidentiality via a secure method that in no way saves or distributes any sort of personal data involved. Feel safe knowing your files are kept protected whenever you use our service!