The DSS-EA-310 form serves as a critical tool for individuals receiving Medical Assistance or Temporary Assistance for Needy Families (TANF) to report any changes in their circumstances. It is designed to ensure that the Department of Social Services is kept up-to-date with accurate and current information that could affect an individual's or a family's benefits. By meticulously filling out this form, recipients are required to report various types of changes, such as adjustments in household composition, income fluctuations, pregnancy, or modifications in health insurance status. Specifically, it covers diverse situations including someone moving into or out of a recipient's home, changes in employment status or income, and alterations in other income or resources like alimony or pension. The form also inquires about new household members' intentions regarding filing federal income tax returns, reflecting its comprehensive approach to capturing all relevant changes. Prompt reporting, within 10 days from the day the change occurred, is emphasized to avoid any potential interruption or inappropriate allocation of benefits. Additionally, the form carries a serious reminder about the implications of providing false information, highlighting the possibility of reduced benefits, repayment obligations, or even criminal prosecution. This underscores the importance of accuracy and honesty in the reporting process. The DSS-EA-310 form, therefore, not only assists in the administrative process of benefit allocation but also plays a crucial role in ensuring fair and lawful distribution of resources among beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Dss Ea 310 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 1st, unearned, TANF, aCHECK |
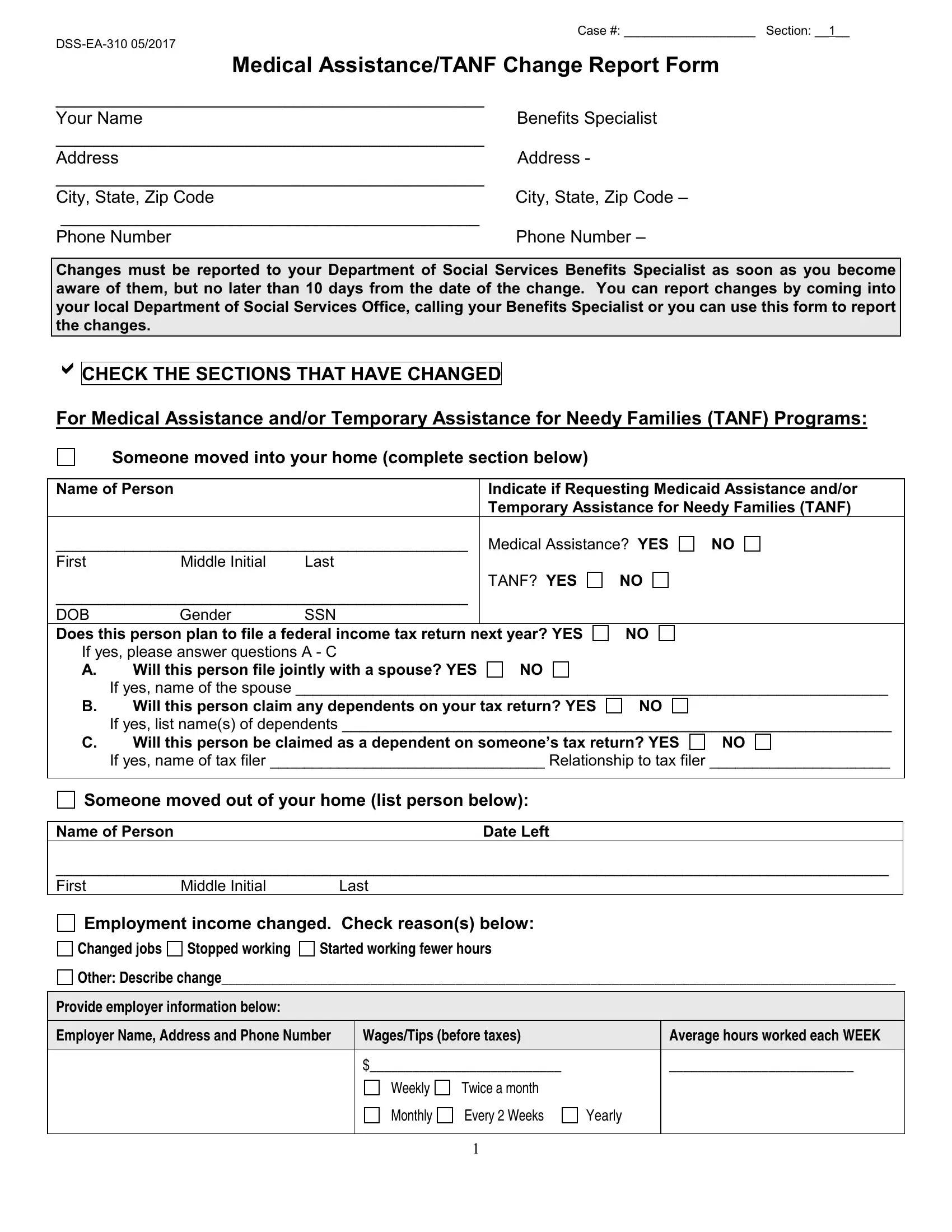
Case #: ___________________ Section: __1__
Medical Assistance/TANF Change Report Form
_____________________________________________ |
|
Your Name |
Benefits Specialist |
_____________________________________________ |
|
Address |
Address - |
_____________________________________________ |
|
City, State, Zip Code |
City, State, Zip Code – |
____________________________________________ |
|
Phone Number |
Phone Number – |
Changes must be reported to your Department of Social Services Benefits Specialist as soon as you become aware of them, but no later than 10 days from the date of the change. You can report changes by coming into your local Department of Social Services Office, calling your Benefits Specialist or you can use this form to report the changes.
CHECK THE SECTIONS THAT HAVE CHANGED
For Medical Assistance and/or Temporary Assistance for Needy Families (TANF) Programs:
Someone moved into your home (complete section below)
Name of Person |
|
Indicate if Requesting Medicaid Assistance and/or |
|||
|
|
|
Temporary Assistance for Needy Families (TANF) |
||
________________________________________________ |
Medical Assistance? YES |
NO |
|||
First |
Middle Initial |
Last |
|
|
|
|
|
|
TANF? YES |
NO |
|
________________________________________________ |
|
|
|
||
DOB |
Gender |
SSN |
|
|
|
Does this person plan to file a federal income tax return next year? YES |
NO |
|
|||
If yes, please answer questions A - C |
|
|
|
||
A. |
Will this person file jointly with a spouse? YES |
NO |
|
|
|
|
If yes, name of the spouse _____________________________________________________________________ |
||||
B. |
Will this person claim any dependents on your tax return? YES |
NO |
|
||
|
If yes, list name(s) of dependents ________________________________________________________________ |
||||
C. |
Will this person be claimed as a dependent on someone’s tax return? YES |
NO |
|||
|
If yes, name of tax filer ________________________________ Relationship to tax filer _____________________ |
||||
|
|
|
|
|
|
Someone moved out of your home (list person below):
Name of PersonDate Left
_________________________________________________________________________________________________
First Middle Initial Last
Employment income changed. Check reason(s) below:
Changed jobs |
Stopped working |
Started working fewer hours |
Other: Describe change_______________________________________________________________________________________________
Provide employer information below:
Employer Name, Address and Phone Number |
Wages/Tips (before taxes) |
|
Average hours worked each WEEK |
|
|
|
|
|
|
|
$___________________________ |
|
__________________________ |
|
|
Weekly |
Twice a month |
|
|
|
Monthly |
Every 2 Weeks |
Yearly |
|
|
|
|
|
|
|
|
1 |
|
|
If
Other income changed. Complete all that apply
Source of Income |
Amount |
How often received? |
Source of Income |
Amount |
How often received? |
Unemployment |
|
|
Alimony Received |
|
|
Pensions |
|
|
Net Farming/fishing |
|
|
Social Security |
|
|
Net rental/royalty |
|
|
Retirement |
|
|
Other income type |
|
|
Accounts |
|
|
|
|
|
Someone in the household is pregnant. If checked, complete questions below:
Name of person that is pregnant: ______________________ Due Date _______ Number of babies ________
Someone gave birth to a child. If checked, complete questions below:
Date of birth: ______________ Name of newborn: _______________________________ Gender: ____________
For Medical Assistance Only:
Health insurance started, stopped, or company changed?
List the policy # ___________________________ Co. Name/address: _____________________________
Describe the change: ______________________________________________________________________
For TANF Only:
CHECK THE SECTION(S) THAT HAVE CHANGED, EXPLAIN & ATTACH PROOF:
Bank accounts/resources changed. Describe new accounts, increased amounts in existing accounts,etc.
___________________________________________________________________________________
Bought, sold, traded, or gave away vehicles (cars, trucks, boats, etc). Describe the change:
_____________________________________________________________________________________
The amount you pay for child support payments started, stopped, or changed. Describe who the payment is for, who it is paid to, and the change in payment:
_____________________________________________________________________________________
School attendance changed. Provide name, change that occurred, and date of occurrence:
____________________________________________________________________________________
I understand that the information on this form is subject to verification by Federal, State and local officials to determine that such information on this form is correct and complete. If any information is found to be incorrect, benefits may be reduced or terminated and I may be responsible for paying the benefits back. I declare and affirm under penalties of perjury that this report form has been examined by me and to the best of my knowledge and belief is in all things true and correct. I understand I may be subject to criminal prosecution for knowingly providing incorrect information.
________________________________________________________ |
___________ |
Signature |
Date |
Additional Comments: _____________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
2