

yyyy can be filled in online with ease. Just use FormsPal PDF editing tool to accomplish the job right away. We at FormsPal are committed to giving you the absolute best experience with our editor by consistently presenting new functions and upgrades. Our editor is now much more intuitive as the result of the latest updates! At this point, filling out documents is a lot easier and faster than before. Should you be looking to get started, here is what it requires:
Step 1: Hit the "Get Form" button at the top of this page to access our editor.
Step 2: After you open the PDF editor, you will find the form all set to be completed. In addition to filling in various blank fields, you may also perform many other things with the Document, specifically writing your own text, modifying the original text, adding illustrations or photos, affixing your signature to the form, and more.
Be attentive while filling in this pdf. Make sure all required areas are done correctly.
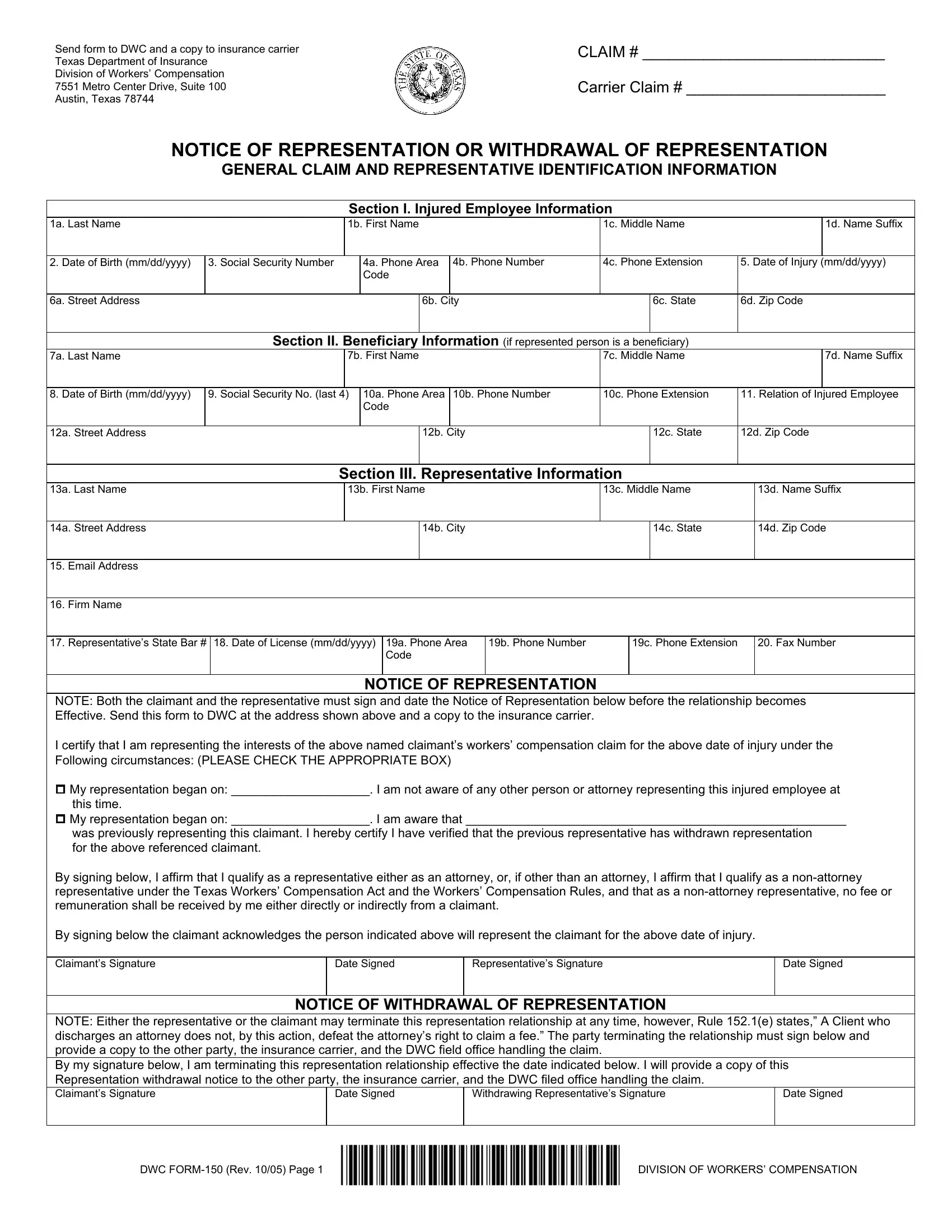
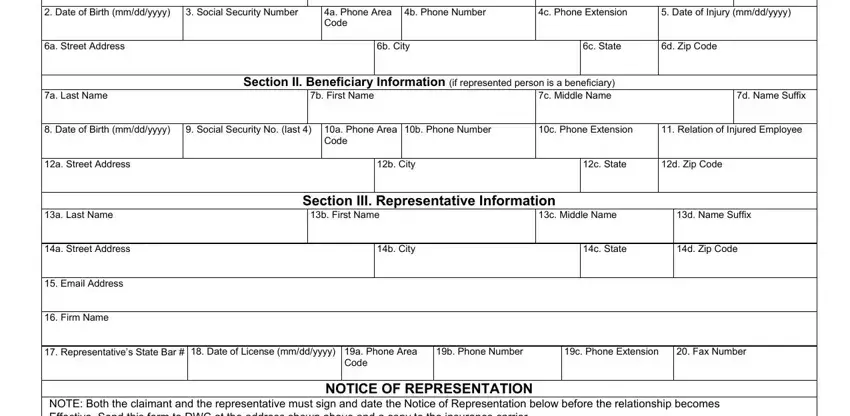
1. Begin filling out your yyyy with a number of necessary fields. Note all the important information and be sure there is nothing forgotten!
2. Once this segment is finished, you'll want to put in the necessary specifics in NOTE Both the claimant and the, Representatives Signature, Date Signed, Date Signed, NOTICE OF WITHDRAWAL OF, NOTE Either the representative or, Withdrawing Representatives, Date Signed, Date Signed, DWC FORM Rev Page, and DIVISION OF WORKERS COMPENSATION allowing you to move forward to the 3rd part.
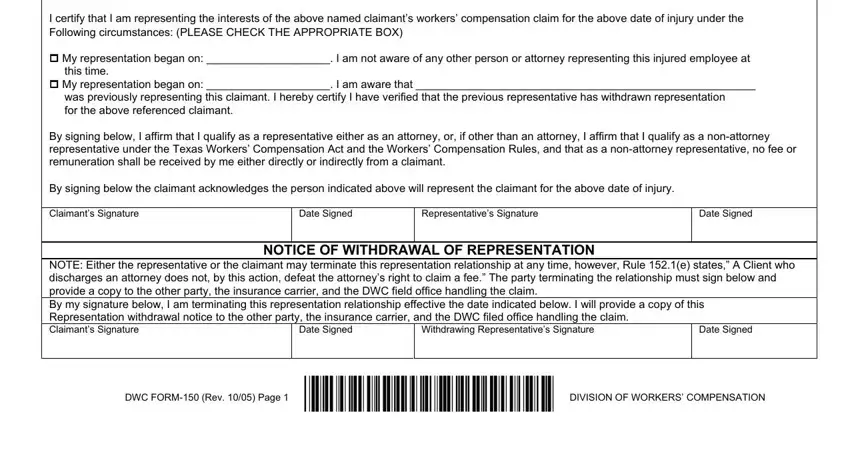
Regarding DIVISION OF WORKERS COMPENSATION and NOTE Both the claimant and the, make sure you review things here. Both of these are definitely the key fields in this file.
Step 3: You should make sure your information is right and press "Done" to complete the project. Sign up with FormsPal now and easily gain access to yyyy, available for downloading. Each change you make is conveniently preserved , which enables you to edit the pdf later anytime. FormsPal is committed to the personal privacy of all our users; we make sure that all information processed by our system is kept secure.