

It is possible to fill out dwc form 73 effortlessly with our PDFinity® online PDF tool. FormsPal expert team is ceaselessly working to expand the editor and enable it to be even better for clients with its many features. Enjoy an ever-improving experience today! All it takes is just a few easy steps:
Step 1: Open the PDF in our editor by clicking the "Get Form Button" at the top of this page.
Step 2: This editor will let you modify nearly all PDF documents in various ways. Change it by including personalized text, correct existing content, and place in a signature - all within a couple of clicks!
Pay attention while filling in this document. Make certain all necessary areas are completed correctly.
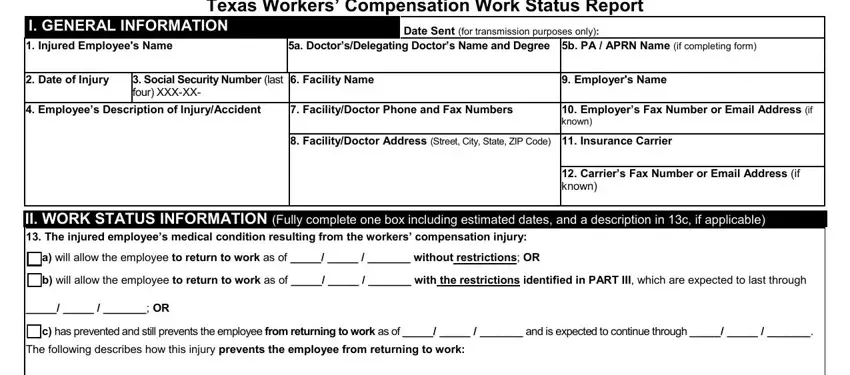
1. It's very important to complete the dwc form 73 accurately, so be mindful when filling in the areas comprising these particular blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - III ACTIVITY RESTRICTIONS Only, Overhead reaching Keyboarding Other, Other, Misc Restrictions if any Max, No drivingoperating heavy, No skin contact with, No running Dressing changes, Left handwrist Right handwrist, Other, Left leg Right leg Back Left, Other Restrictions if any, LiftCarry Restrictions if any, May not liftcarry objects more, than hours per day, and May not perform any liftingcarrying with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
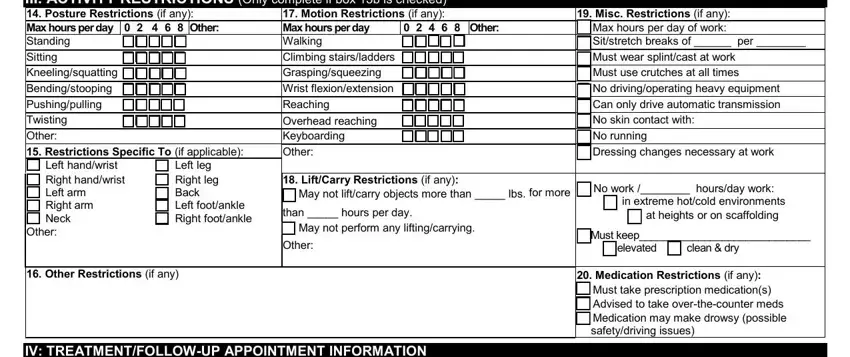
Always be very attentive when filling out III ACTIVITY RESTRICTIONS Only and LiftCarry Restrictions if any, because this is the section in which most users make some mistakes.
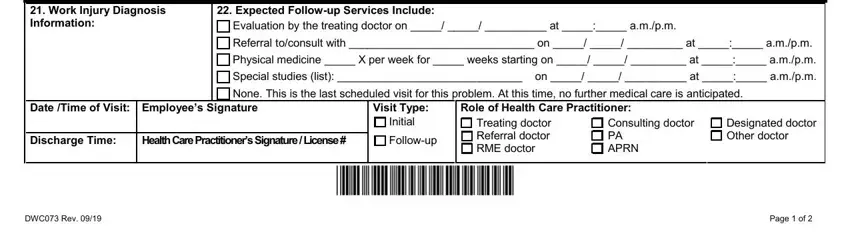
3. This subsequent part is considered fairly easy, IV TREATMENTFOLLOWUP APPOINTMENT, Evaluation by the treating doctor, Date Time of Visit Employees, Visit Type, Role of Health Care Practitioner, Discharge Time, Health Care Practitioners, Followup, Initial, Treating doctor Referral doctor, Consulting doctor PA APRN, Designated doctor Other doctor, DWC Rev, and Page of - these form fields will have to be filled out here.
Step 3: Before finishing this form, double-check that blank fields have been filled out correctly. Once you believe it's all fine, click “Done." Download your dwc form 73 when you sign up for a free trial. Easily get access to the pdf form in your personal cabinet, together with any modifications and changes being all preserved! At FormsPal, we aim to be certain that your information is stored private.