
Our PDF editor works to make completing files trouble-free. It is really convenient to enhance the [FORMNAME] form. Try out these steps if you need to do this:
Step 1: Choose the button "Get form here" to open it.
Step 2: So you should be on the form edit page. You'll be able to add, customize, highlight, check, cross, add or remove areas or text.
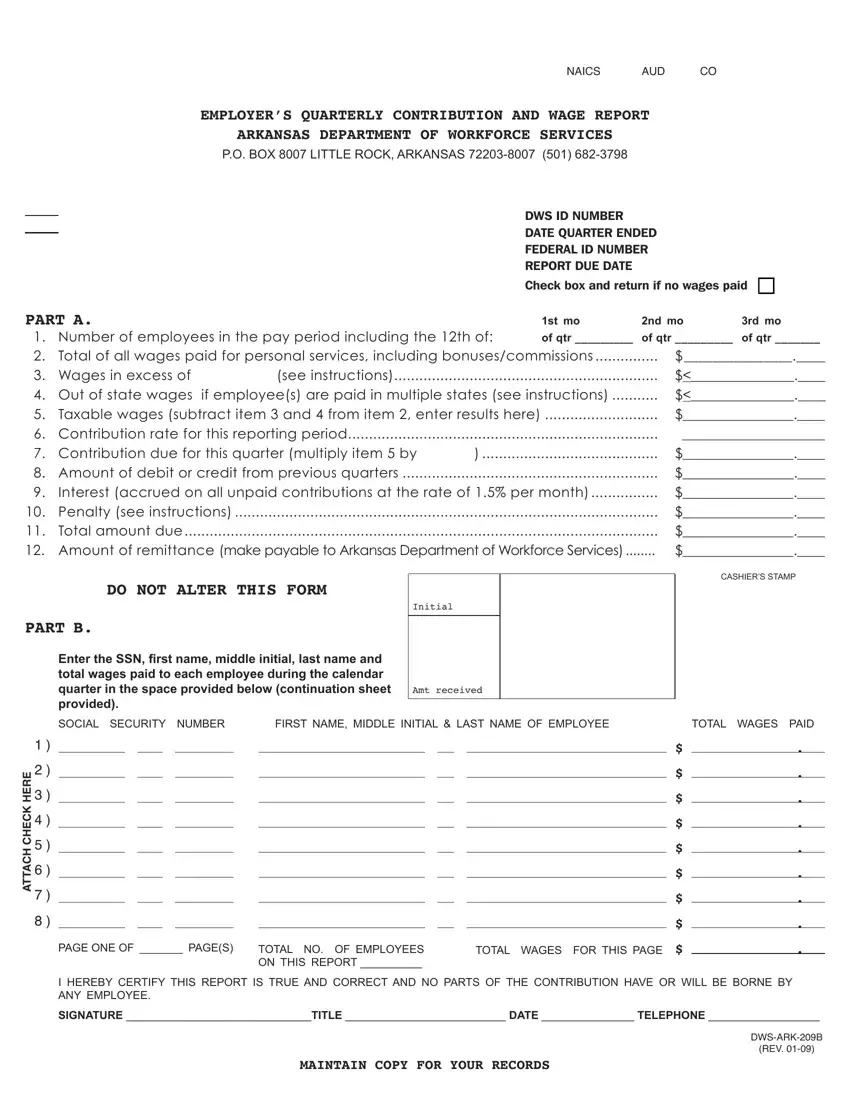
Provide the appropriate content in every single section to fill out the PDF arkansas employer form
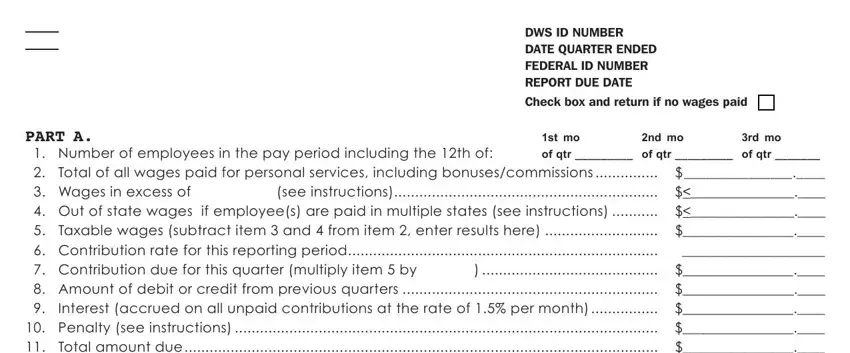
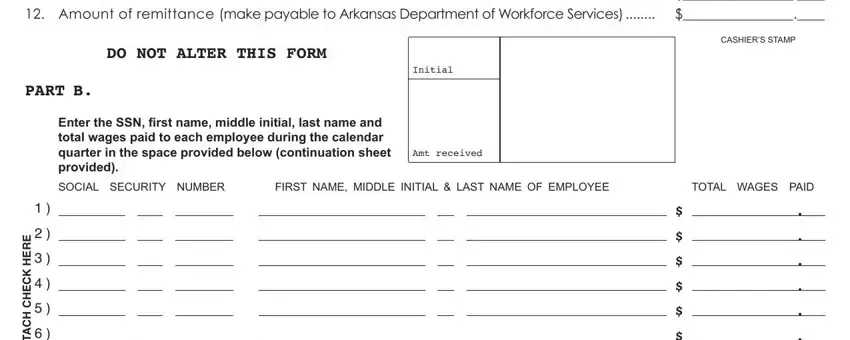
Write down the appropriate details in PART A Number of employees in the, DO NOT ALTER THIS FORM, Initial, PART B, Enter the SSN irst name middle, Amt received, CASHIERS STAMP, SOCIAL SECURITY NUMBER, FIRST NAME MIDDLE INITIAL LAST, TOTAL WAGES PAID, and E R E H K C E H C H C A T T A part.
Indicate the vital data in E R E H K C E H C H C A T T A, PAGE ONE OF PAGES, TOTAL NO OF EMPLOYEES ON THIS, TOTAL WAGES FOR THIS PAGE, I HEREBY CERTIFY THIS REPORT IS, SIGNATURE TITLE DATE TELEPHONE, MAINTAIN COPY FOR YOUR RECORDS, and DWSARKB REV box.
Take the time to include the rights and obligations of the parties within the CONTINUATION SHEET FOR FORM B, DWS ID Number, Quarter End Date, Employer, Town, Page of, SOCIAL SECURITY NUMBER, FIRST NAME MIDDLE INITIAL LAST, and TOTAL WAGES PAID space.
Finalize the template by analyzing all of these sections: .
Step 3: As you click the Done button, your completed file is readily exportable to each of your devices. Alternatively, you will be able to deliver it using email.
Step 4: Make sure you keep away from potential problems by producing as much as 2 duplicates of the form.
