
In case you desire to fill out form 766 r disability application, you don't have to install any kind of software - simply use our online PDF editor. The editor is continually maintained by us, receiving powerful features and turning out to be greater. If you're seeking to begin, here's what it requires:
Step 1: First of all, access the pdf editor by pressing the "Get Form Button" above on this site.
Step 2: As soon as you launch the online editor, you will get the form all set to be filled out. Apart from filling in different blank fields, you may also do other actions with the PDF, particularly adding custom text, changing the initial text, adding images, affixing your signature to the document, and more.
This form will involve specific details; in order to guarantee consistency, don't hesitate to take note of the next steps:
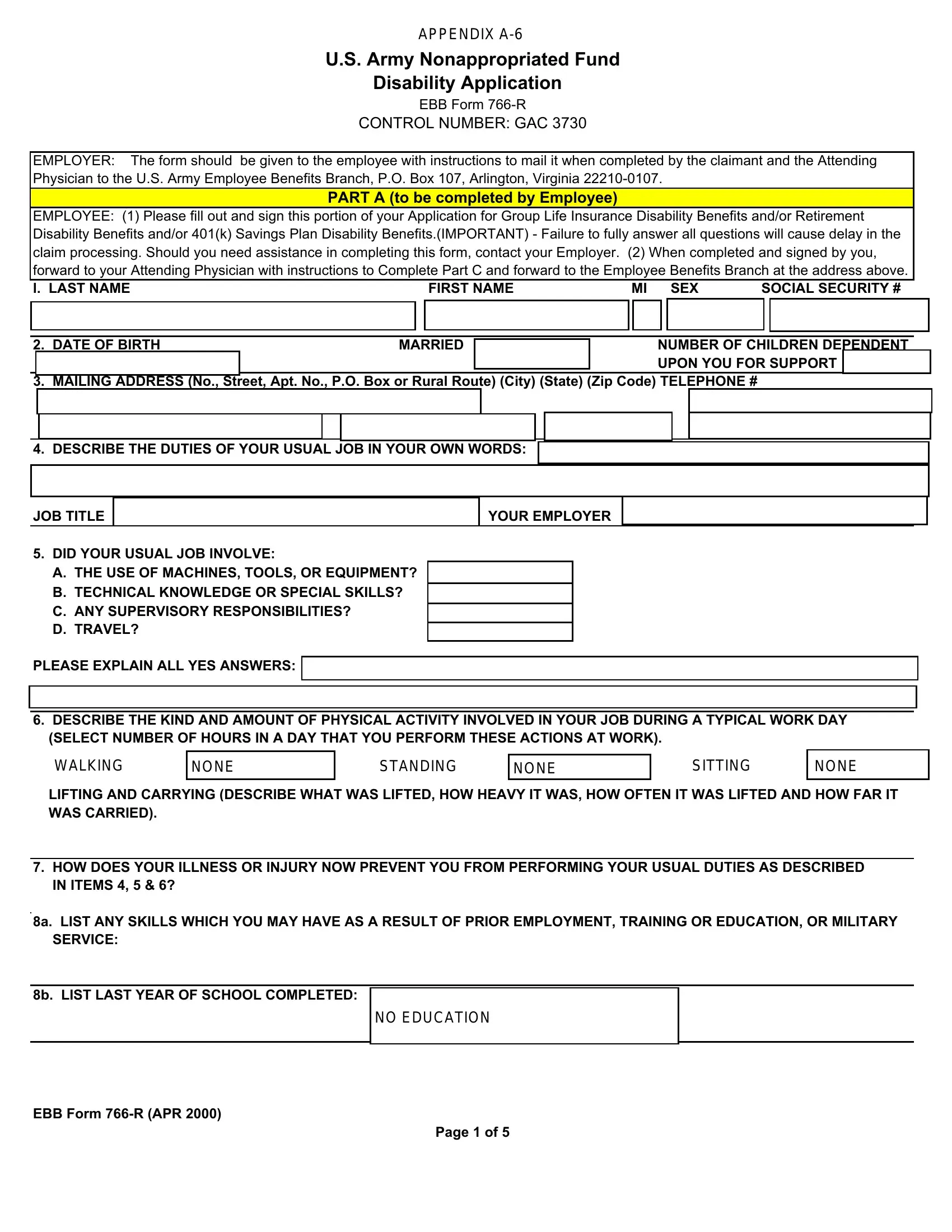
1. The form 766 r disability application will require specific information to be entered. Ensure the next fields are complete:
2. Just after completing the last section, head on to the next step and fill in all required details in all these blanks - DID YOUR USUAL JOB INVOLVE A THE, PLEASE EXPLAIN ALL YES ANSWERS, DESCRIBE THE KIND AND AMOUNT OF, LIFTING AND CARRYING DESCRIBE WHAT, HOW DOES YOUR ILLNESS OR INJURY, a LIST ANY SKILLS WHICH YOU MAY, and b LIST LAST YEAR OF SCHOOL.
People frequently make errors while filling out DID YOUR USUAL JOB INVOLVE A THE in this area. Ensure that you read twice whatever you enter right here.
3. Your next part is normally hassle-free - fill out all the blanks in BEFORE YOU STOPPED WORKING DID, BRIEFLY DESCRIBE YOUR INJURY OR, IF CONDITION DUE TO INJURY PLEASE, WHERE DID IT OCCUR, DESCRIBE HOW ACCIDENT OCCURRED, WHAT WAS YOUR LAST DAY OF WORK, IF YOU ARE NO LONGER DISABLED, DATE OF FIRST TREATMENT FOR THIS, and LIST THE NAME ADDRESS AND to conclude this process.
4. To go ahead, this fourth step will require typing in a handful of form blanks. Included in these are LIST THE NAME ADDRESS AND, HOW OFTEN DO YOU SEE THIS, DATE OF LAST VISIT, REASONS FOR VISITS, TYPE OF TREATMENT RECEIVED, HAVE YOU SEEN ANY OTHER DOCTOR, DATE OF LAST VISIT, REASONS FOR VISITS, TYPE OF TREATMENT RECEIVED, and HAS YOUR DOCTOR TOLD YOU TO, which are crucial to going forward with this document.
5. Since you approach the last parts of your form, there are actually just a few extra things to undertake. Specifically, EBB FORM RAPR, and Page of should all be filled out.
Step 3: Go through all the details you've inserted in the blanks and click on the "Done" button. Right after setting up a7-day free trial account here, it will be possible to download form 766 r disability application or email it right off. The file will also be available via your personal account menu with all of your changes. FormsPal is dedicated to the privacy of all our users; we always make sure that all information processed by our editor is kept protected.