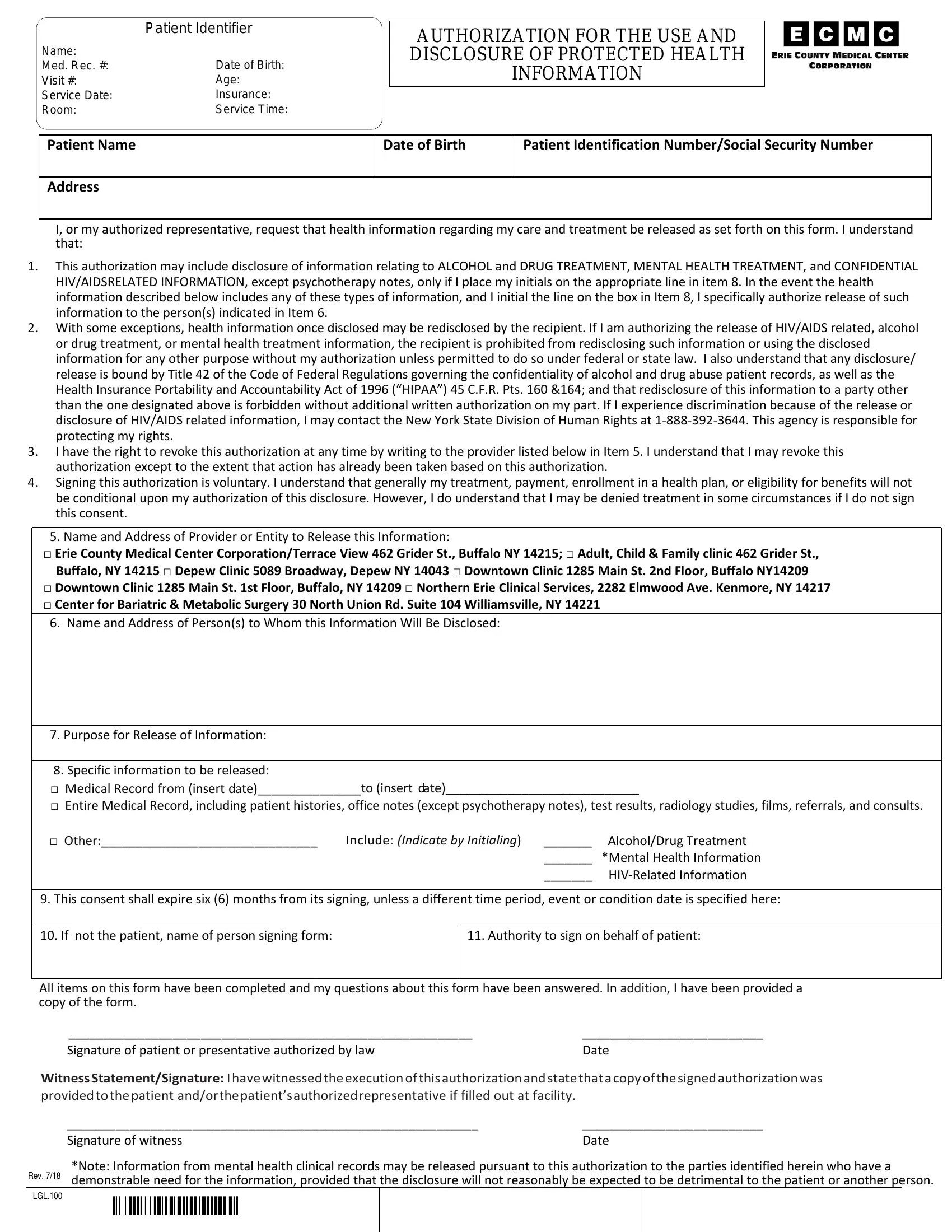
In an era where personal health information is both highly sensitive and crucially important, the ECMC Authorization Form plays a vital role in the management and sharing of one's medical records. This comprehensive document meticulously outlines how a patient's health information—ranging from basic medical history to specific details about drug treatment, mental health care, and confidential HIV/AIDS-related data—can be used and disclosed responsibly. By initiating this form, a patient or their authorized representative grants permission for the release of their medical information under terms that respect their privacy and comply with regulatory statutes like HIPAA. Importantly, the form also touches on the authority to include information about alcohol and drug treatment or mental health details, subject to the patient's explicit consent. The inclusion of options for revoking authorization, understanding the voluntary nature of the agreement, and detailing the provider or entity responsible for releasing information underscores the patient's control over their information. Recipients of the disclosed information are bound by specific legal and ethical restrictions, preventing further disclosure without explicit consent, a safeguard especially pertinent for sensitive information. The document also lists service locations and introduces potential costs associated with obtaining records, noting exceptions for continuity of care. By agreeing to the terms, patients navigate a delicate balance between the need for information sharing for improved healthcare delivery and the imperative to protect their privacy and rights.
| Question | Answer |
|---|---|
| Form Name | Ecmc Authorization Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ecmc form, ecmc medical records, kettering health org authorization for disclosure of protected health infor, ecmc |
