There isn't anything difficult concerning completing the de1000m once you begin using our tool. Following these simple steps, you will have the fully filled out PDF document within the shortest period you can.
Step 1: Click the "Get Form Here" button.
Step 2: You are now on the form editing page. You can edit, add text, highlight specific words or phrases, place crosses or checks, and insert images.
To be able to create the de1000m PDF, provide the details for all of the parts:
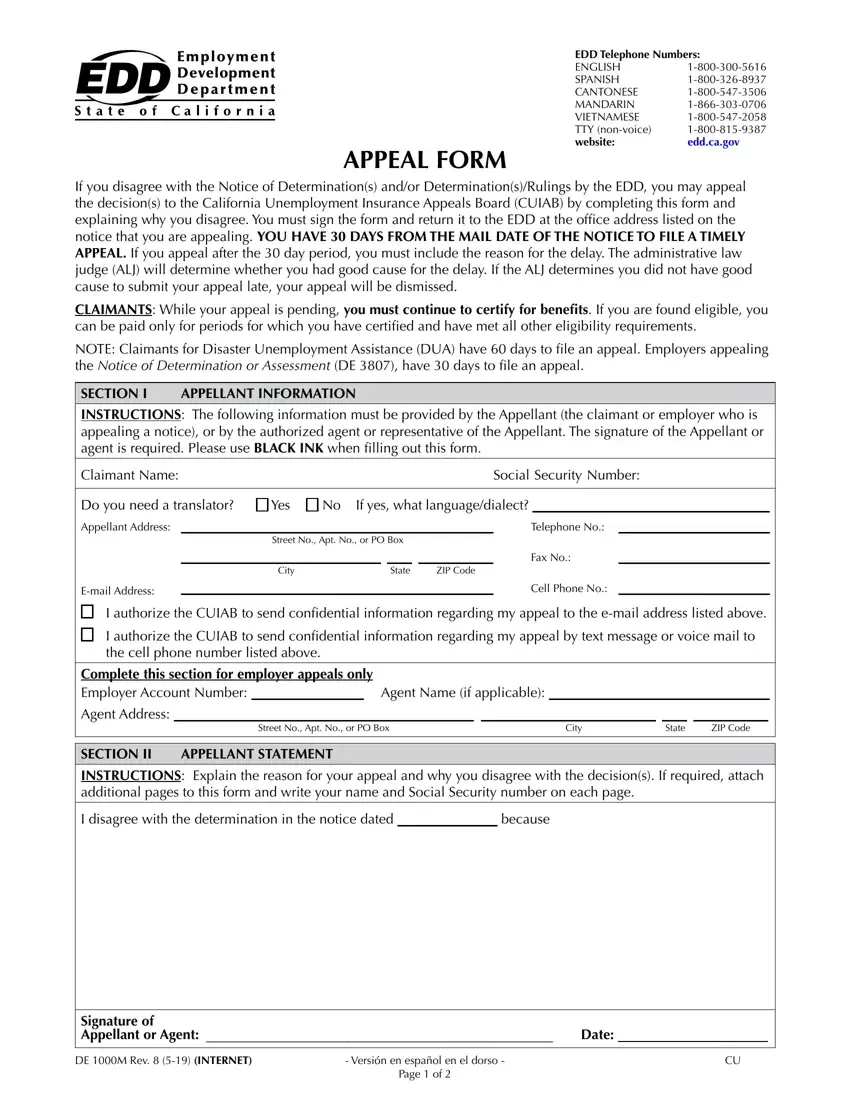
In the I authorize the CUIAB to send, I authorize the CUIAB to send, Complete this section for employer, Agent Name if applicable, Street No Apt No or PO Box, City, State, ZIP Code, SECTION II, APPELLANT STATEMENT, INSTRUCTIONS Explain the reason, I disagree with the determination, and because area, put in writing your details.
Inside the section referring to Signature of Appellant or Agent, DE M Rev INTERNET, and Versión en español en el dorso, it's essential to put down some demanded data.

The Números de Teléfono del EDD INGLÉS, eddcagov, FORMULARIO DE APELACIÓN, Si usted no está de acuerdo con la, SOLICITANTES DE BENEFICIOS, NOTA Los solicitantes de, SECCIÓN I, INFORMACIÓN DEL APELANTE, INSTRUCCIONES La siguiente, Nombre del Solicitante, Número de Seguro Social, Necesita un traductor, Si marcó sí para qué idiomadialecto, Dirección del Apelante, and N de Teléfono section is where either side can place their rights and obligations.
Review the areas Dirección del Apelante, N de calle N de Apto o Apartado, Dirección de Correo Electrónico, Ciudad, Estado Código Postal, N de Teléfono, N de Fax, N de Teléfono Celular, Autorizo a la Junta de Apelaciones, apelación a la dirección de correo, Autorizo a la Junta de Apelaciones, apelación por medio de mensaje de, Complete esta sección para, Nombre del Agente si aplica, and N de calle N de Apto o Apartado and thereafter fill them in.
Step 3: Click the Done button to save your document. Now it is offered for upload to your gadget.
Step 4: It is better to prepare copies of the file. There is no doubt that we are not going to disclose or check out your information.
