



It is possible to fill out new york emedny 436701 effortlessly with the help of our PDF editor online. To make our tool better and more convenient to use, we consistently come up with new features, bearing in mind feedback from our users. If you are looking to begin, this is what it takes:
Step 1: Simply click on the "Get Form Button" above on this webpage to access our pdf file editing tool. There you'll find all that is necessary to work with your file.
Step 2: The editor will let you change your PDF form in a range of ways. Enhance it by writing customized text, adjust existing content, and include a signature - all readily available!
This form will need specific data to be filled out, hence you need to take whatever time to type in precisely what is asked:
1. Complete the new york emedny 436701 with a group of major fields. Get all of the necessary information and ensure not a single thing missed!
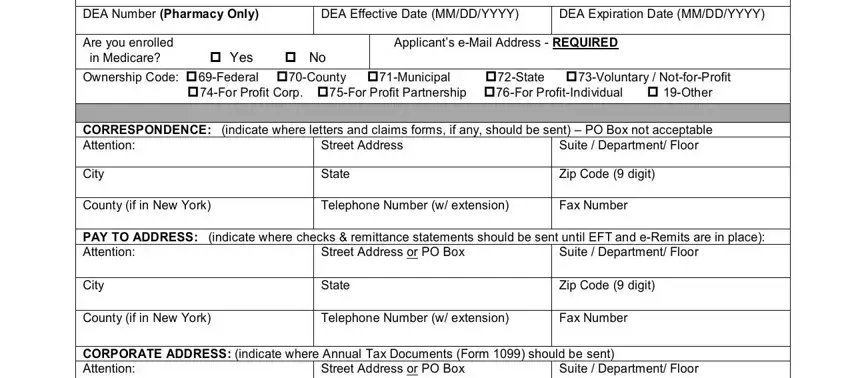
2. The next step would be to complete all of the following blank fields: DEA Number Pharmacy Only, DEA Effective Date MMDDYYYY, DEA Expiration Date MMDDYYYY, Are you enrolled in Medicare Yes, Applicants eMail Address REQUIRED, CORRESPONDENCE indicate where, Suite Department Floor, Street Address, City, State, Zip Code digit, County if in New York, Telephone Number w extension, Fax Number, and PAY TO ADDRESS indicate where.
3. This next portion will be focused on City, State, Zip Code digit, County if in New York, Telephone Number w extension, eMail Address REQUIRED, and EMEDNY - fill out each of these fields.
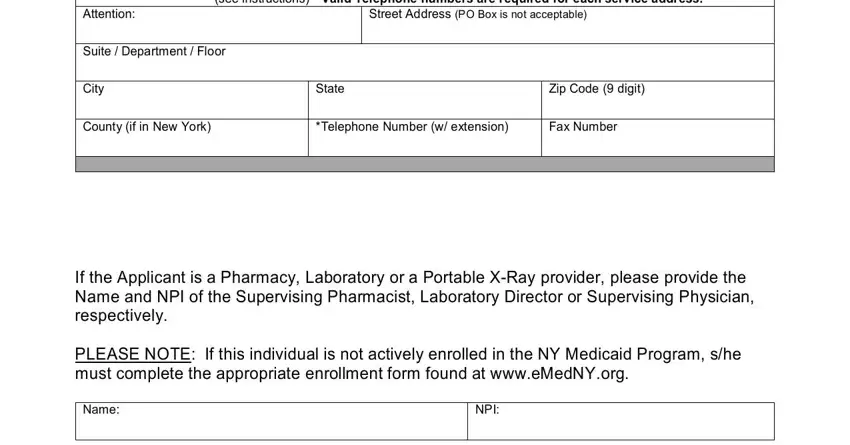
4. To go onward, this step involves typing in a couple of blanks. Included in these are SERVICE ADDRESS where service is, Street Address PO Box is not, Suite Department Floor, City, State, Zip Code digit, County if in New York, Telephone Number w extension, Fax Number, If the Applicant is a Pharmacy, Name, and NPI, which are vital to continuing with this particular form.
5. Now, the following final section is precisely what you need to complete before closing the form. The fields in this case include the following: Completion is required by CFR, Entity Name, FEIN, NPI if exempt leave blank, Ownership in Applicant per CFR, Name of Individual or Entity, Title if individual, Date of Birth if individual, Address Home Address if Individual, City State Zip Code digit, SSN for individual, FEIN for entity, of Ownership if none put, NPI or NY Medicaid ID if none, and For Individuals Only If you are.
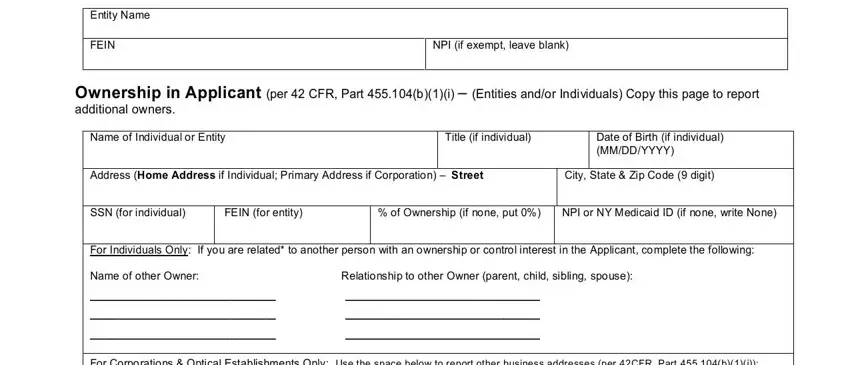
Concerning FEIN for entity and Ownership in Applicant per CFR, make certain you take a second look in this current part. Those two are viewed as the most important ones in this document.
Step 3: Once you've reread the information entered, just click "Done" to conclude your form at FormsPal. Grab your new york emedny 436701 once you register at FormsPal for a 7-day free trial. Immediately gain access to the form inside your FormsPal account, along with any modifications and adjustments all preserved! We don't share or sell any information you type in whenever dealing with forms at FormsPal.