The physical form for work filling out procedure is effortless. Our PDF tool lets you work with any PDF document.
Step 1: You can choose the orange "Get Form Now" button at the top of the webpage.
Step 2: Now you are going to be on your file edit page. You can include, modify, highlight, check, cross, add or remove areas or words.
These segments will create the PDF form that you'll be filling in:
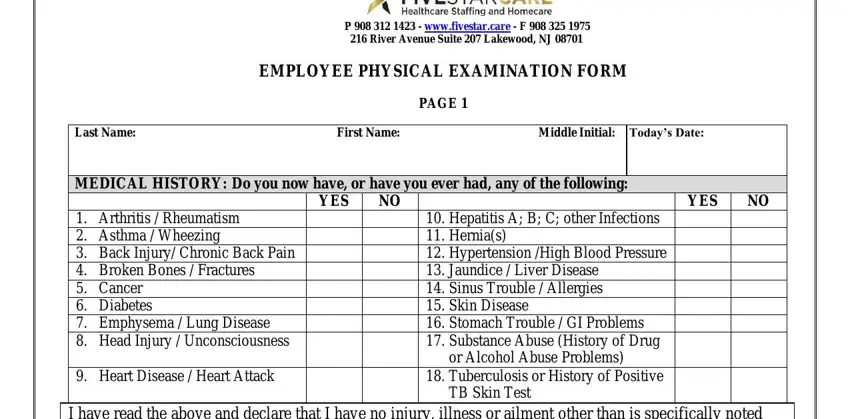
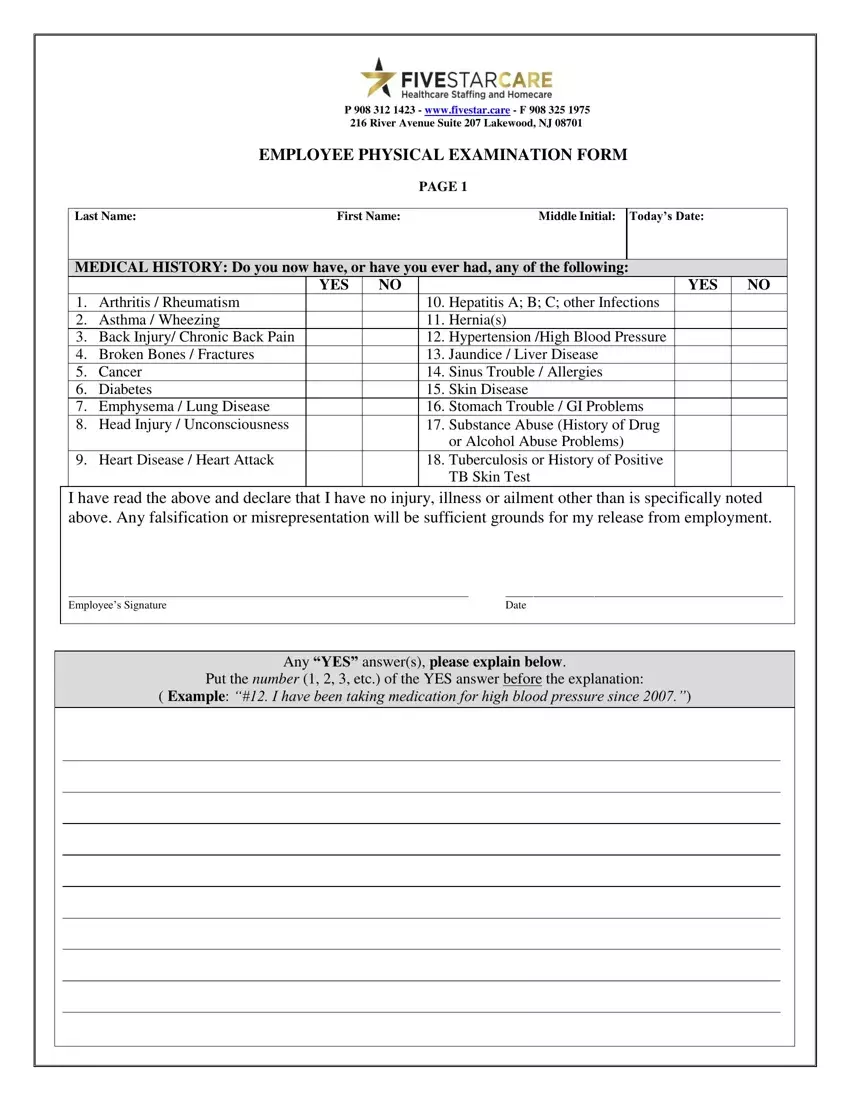
Write the appropriate data in the Employees Signature, Date, and Any YES answers please explain area.
Put together the essential particulars in the P wwwfivestarcare F River, EMPLOYEE PHYSICAL EXAMINATION FORM, PAGE, Last Name, First Name, Middle Initial, Todays Date, Job Title, DOB, Age, Sex, Temp, Pulse, Resp, and DrugFood Allergies section.
Feel free to place the rights and responsibilities of the parties inside the PHYSICAL EXAM General Appearance, Psychiatric tics stuttering nail, Physicians review of persons, PPD Mantoux Test for Tuberculosis, Result, nd Step Date, Result, Chest XRay Date Performed, Results, THIS APPLICANT IS FIT FOR, and Deferred for Functional Capacity space.
Look at the fields Examining Physicians Signature, and Date Physical Examination Performed and next fill them in.

Step 3: When you are done, click the "Done" button to upload the PDF form.
Step 4: Generate copies of your file - it will help you stay away from possible future problems. And don't be concerned - we don't distribute or view your information.
