
Through the online PDF tool by FormsPal, you can easily complete or modify cal choice termination form right here. We are aimed at giving you the best possible experience with our editor by regularly releasing new features and improvements. With all of these improvements, working with our editor becomes better than ever! All it takes is a couple of easy steps:
Step 1: Hit the "Get Form" button above. It will open our pdf editor so you could start filling out your form.
Step 2: With our state-of-the-art PDF tool, you can do more than merely complete forms. Edit away and make your documents seem sublime with custom textual content put in, or fine-tune the original input to excellence - all accompanied by the capability to add stunning pictures and sign the document off.
This PDF form will require some specific information; to ensure accuracy, you need to take note of the recommendations down below:
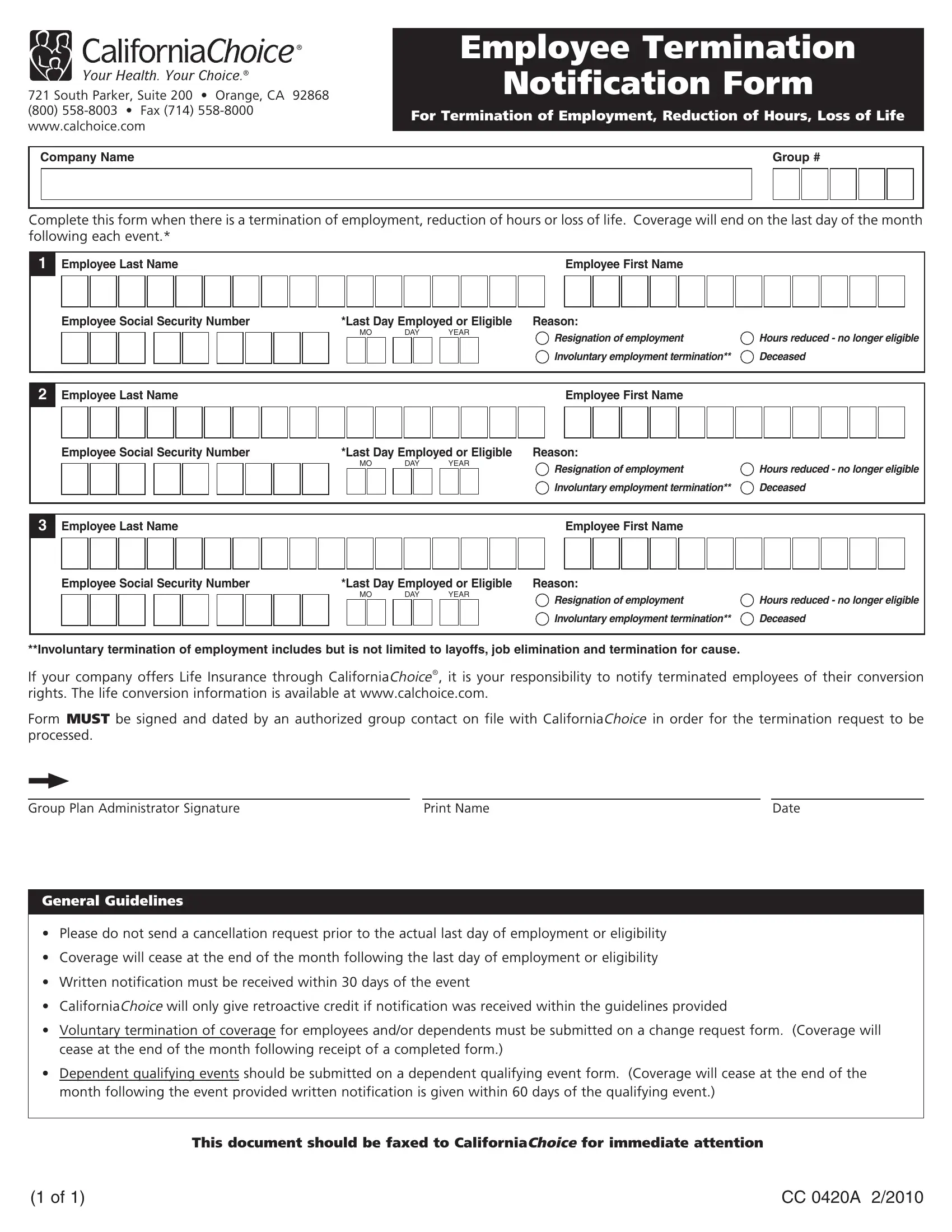
1. Begin completing the cal choice termination form with a selection of essential fields. Note all of the information you need and make sure nothing is omitted!
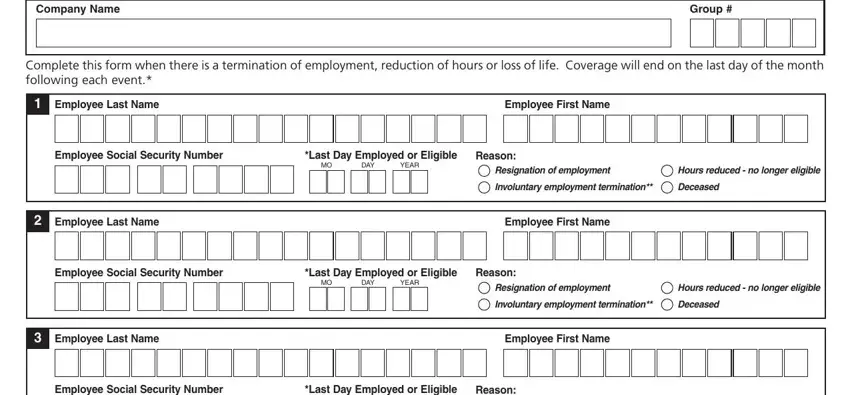
2. After this part is completed, proceed to enter the suitable details in these - Employee Social Security Number, Last Day Employed or Eligible, Reason, DAY, YEAR, Resignation of employment, Hours reduced no longer eligible, Involuntary employment termination, Deceased, Involuntary termination of, If your company offers Life, Form MUST be signed and dated by, Group Plan Administrator Signature, Print Name, and Date.
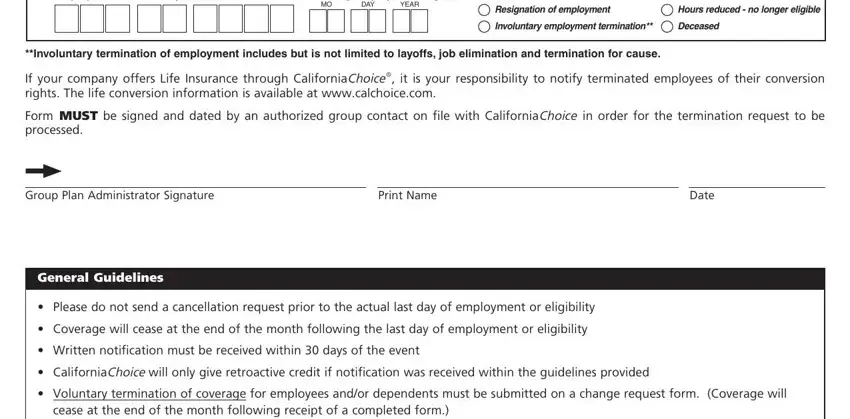
It is easy to get it wrong when filling out the Reason, so make sure to go through it again before you finalize the form.
Step 3: Right after you have reread the information you filled in, just click "Done" to complete your form. Join us right now and instantly get cal choice termination form, available for download. Each and every modification you make is conveniently saved , which enables you to change the document at a later stage if required. When you use FormsPal, you're able to fill out documents without the need to worry about information incidents or records getting distributed. Our secure system ensures that your private information is maintained safely.